Our teeth, those sturdy tools for chewing and vital components of a bright smile, are more complex than they appear on the surface. Deep within the hard outer layers of enamel and dentin lies a soft, living core known as the dental pulp. This inner sanctum is the tooth’s very life force, and when a tooth sustains damage, the pulp is often the first to sound the alarm and, unfortunately, the first to suffer serious consequences if the problem isn’t addressed.
The Hidden World: Understanding Dental Pulp
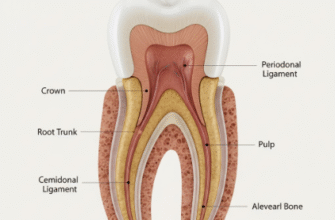
Imagine a tiny, secure chamber right in the heart of your tooth. That’s the pulp chamber, extending down into the roots through narrow passages called root canals. This chamber isn’t empty; it’s bustling with activity. The pulp itself is a delicate, gelatinous tissue composed of several key elements:
- Nerves: These are branches of larger nerves in your jaw. Their primary job here is to sense stimuli, most notably temperature (hot and cold) and pressure. When you feel a sudden twinge from ice cream or a dull ache, it’s these nerves signaling a potential issue.
- Blood Vessels: A network of tiny arteries and veins supplies the pulp with oxygen and nutrients, essential for keeping the cells within alive and functioning. They also carry away waste products.
- Connective Tissue: This forms the structural framework of the pulp, holding everything together. It includes specialized cells like fibroblasts (which create fibers) and odontoblasts.
- Odontoblasts: These are remarkable cells lining the outer edge of the pulp, right next to the dentin. Their primary role throughout life is to produce dentin. If the tooth is irritated, they can lay down more dentin (reparative dentin) as a protective measure.
- Immune Cells: Like elsewhere in the body, the pulp has defense cells, such as macrophages and lymphocytes, ready to respond to threats like invading bacteria.
The pulp, therefore, serves multiple crucial functions: it provides sensation, nourishes the dentin, forms new dentin when needed, and mounts a defense against infection. It’s a dynamic, living tissue, but its location within rigid, unyielding walls of dentin also makes it vulnerable.
The Onslaught: How Tooth Damage Reaches the Pulp
Several pathways can lead to pulp irritation and damage. The most common culprits breach the tooth’s protective outer layers, allowing irritants or bacteria to get perilously close to, or directly into, the pulp chamber.
Deep Dental Caries (Cavities)
This is perhaps the most frequent offender. Dental caries begin when bacteria in plaque metabolize sugars from our diet, producing acids. These acids gradually dissolve the enamel, the tooth’s hard outer shell. If left unchecked, the decay progresses deeper, through the softer dentin layer. Dentin is porous, containing microscopic tubules that run directly from the enamel-dentin junction to the pulp. As decay gets closer to the pulp, bacterial toxins and byproducts can seep through these tubules, triggering an inflammatory response in the pulp even before the bacteria physically arrive.
Cracks and Fractures
A sudden impact, biting down on something unexpectedly hard, or even habitual teeth grinding can cause cracks or fractures in a tooth. These can range from tiny craze lines in the enamel to deeper fractures that extend into the dentin or even directly into the pulp. A fracture provides a direct superhighway for bacteria and oral fluids to access the pulp, leading to rapid and severe inflammation.
Trauma
A blow to the mouth, whether from a sports injury, a fall, or an accident, can cause significant damage. The force might not always break the tooth visibly, but it can disrupt the delicate blood supply at the tip of the root (the apex). If the blood supply is severed, the pulp tissue can die due to lack of oxygen and nutrients, even without bacterial invasion initially. Sometimes, trauma causes an immediate inflammatory response due to the physical shock.
Repeated Dental Procedures
While dental treatments aim to fix problems, the procedures themselves can sometimes stress the pulp. Each time a tooth is drilled for a filling or a crown, there’s a degree of irritation to the pulp from heat, vibration, or drying. Usually, the pulp recovers. However, if a tooth undergoes multiple procedures over time, the cumulative stress can sometimes push the pulp beyond its ability to heal, leading to chronic inflammation or eventual death.
The Pulp’s Initial Defense: Inflammation (Pulpitis)
When the pulp senses an attack, whether from bacterial toxins, temperature extremes seeping through thin dentin, or physical trauma, its first line of defense is inflammation. This process, known as pulpitis, is similar to inflammation elsewhere in the body but with a critical difference: the pulp is encased in a rigid, unexpandable chamber.
Here’s what happens during pulpitis:
- Vasodilation: Blood vessels within the pulp widen (dilate) to increase blood flow to the area. This brings more oxygen, nutrients, and importantly, defensive cells to fight off invaders or repair damage.
- Increased Permeability: The walls of these blood vessels become more permeable, allowing fluid and plasma proteins to leak out into the surrounding pulp tissue. Immune cells also migrate out of the vessels into the tissue.
- Swelling (Edema): This leakage of fluid causes the pulp tissue to swell. Elsewhere in the body, swelling has room to expand. In the tooth, however, the hard dentin walls offer no give.
- Increased Pressure: As the pulp swells within its confined space, the internal pressure (intrapulpal pressure) rises significantly.
- Nerve Compression and Pain: This increased pressure squeezes the nerve fibers within the pulp. Inflammatory mediators (chemicals released during inflammation, like prostaglandins and bradykinin) also directly stimulate these nerve endings or make them more sensitive. The result is pain – the tooth’s way of signaling that something is seriously wrong.
Reversible Pulpitis: A Chance for Recovery
If the irritation is mild and short-lived, and the cause is removed (for example, a small cavity is filled), the pulp may be able to recover. This is called reversible pulpitis. The inflammation subsides, blood flow returns to normal, and the pressure decreases. Symptoms of reversible pulpitis typically include:
- Sharp, quick pain, often triggered by cold or sweet foods/drinks.
- Pain that disappears within seconds of the stimulus being removed.
- No spontaneous pain (pain that occurs without any apparent trigger).
At this stage, prompt dental attention to remove the source of irritation is crucial for saving the pulp’s vitality.
Irreversible Pulpitis: The Point of No Return
If the irritation is severe, prolonged, or the bacterial invasion is extensive, the inflammation becomes overwhelming. The increased pressure can become so high that it chokes off the pulp’s own blood supply by collapsing the delicate venules (small veins) at the root tip, preventing blood from exiting. This leads to a vicious cycle: more inflammation, more pressure, less blood flow, more tissue damage. This stage is known as irreversible pulpitis. The pulp tissue is so damaged that it cannot heal, even if the original cause is removed.
Symptoms of irreversible pulpitis are often more intense and persistent:
- Dull, throbbing, or aching pain that can be spontaneous.
- Pain that lingers for minutes or even hours after a stimulus (especially heat, but sometimes cold initially) is removed.
- Pain that may wake you up at night.
- Pain that can be difficult to pinpoint to a specific tooth, sometimes referring to other areas of the jaw or head.
- Sometimes, paradoxically, cold might temporarily relieve the pain by causing vasoconstriction and slightly reducing intrapulpal pressure.
Once pulpitis becomes irreversible, the pulp tissue is destined to die.
Important Note: Ignoring dental pain, especially if it’s spontaneous, lingering, or wakes you at night, can lead to more serious complications. Early assessment by a dental professional is key when a tooth starts signaling distress. Waiting can allow a potentially reversible issue to become irreversible and more complex to manage.
The Demise: Pulp Necrosis
If irreversible pulpitis is left untreated, the compromised blood flow and ongoing assault from bacteria and their toxins eventually lead to the death of the pulp tissue. This is called pulp necrosis. The once vibrant pulp chamber and root canals become a space filled with dead tissue, bacteria, and inflammatory byproducts.
At this stage, the tooth may, ironically, become temporarily asymptomatic regarding temperature sensitivity because the nerves within the pulp are no longer functioning. However, the problem is far from over. The necrotic tissue provides an ideal breeding ground for bacteria, particularly anaerobic bacteria (those that thrive in low-oxygen environments). These bacteria multiply and release potent toxins and enzymes that can cause further damage.
A tooth with a necrotic pulp might exhibit other signs:
- Discoloration: The tooth may gradually turn darker, often grayish, brownish, or yellowish, due to the breakdown of blood products within the dentinal tubules.
- Lack of response to vitality tests: Dentists use tests like applying cold or a mild electric current to check pulp responsiveness. A necrotic pulp will not respond.
The Infection Spreads: Beyond the Tooth’s Confines
The infection doesn’t necessarily stay contained within the dead tooth. Bacteria and their toxins can, and often do, seep out through the small opening(s) at the tip of the root(s) – the apical foramen – into the surrounding bone and tissues. This leads to a new set of problems:
Apical Periodontitis
When the infection reaches the tissues around the root apex (the periapical area), it causes inflammation of the periodontal ligament (the fibers that hold the tooth in its socket) and the surrounding alveolar bone. This is known as apical periodontitis. This can be acute (sudden onset, severe symptoms) or chronic (long-standing, milder or no symptoms).
Symptoms of acute apical periodontitis often include:
- Severe pain when biting or chewing on the tooth.
- The tooth may feel “high” or extruded from its socket.
- Tenderness when the gum tissue over the root is touched.
- Sometimes, visible swelling of the gums or even the face.
Chronic apical periodontitis might be asymptomatic or cause only mild, intermittent discomfort. However, an X-ray will often reveal a dark area (radiolucency) at the root tip, indicating bone loss as the body tries to deal with the persistent infection.
Dental Abscess
If the infection becomes well-established and the body’s defenses are overwhelmed, a collection of pus can form at the root tip. This is a dental abscess (specifically, a periapical abscess). Pus is a mixture of dead white blood cells, dead tissue, bacteria, and inflammatory exudate. An abscess creates pressure, leading to intense, throbbing pain. The infection may try to find a path to drain, sometimes forming a pimple-like fistula (a sinus tract) on the gum, through which pus can ooze out, often providing temporary relief from the pressure and pain.
Other signs of an abscess can include:
- Swelling of the gum, cheek, or jaw.
- Fever.
- Swollen lymph nodes in the neck.
- A general feeling of being unwell (malaise).
An untreated dental abscess can, in rare cases, lead to more widespread and serious infections if bacteria enter the bloodstream or spread to other areas of the head and neck.
Bone Resorption
The chronic inflammation and infection around the root tip stimulate cells called osteoclasts, which are responsible for breaking down bone tissue. This leads to a gradual loss of the bone supporting the tooth. On an X-ray, this appears as a dark shadow around the apex of the root. If significant bone is lost, the tooth can eventually become loose.
The Tooth’s Structure After Pulp Death
Even if the infection is contained or treated, a tooth that has lost its pulp vitality undergoes changes. Without its internal blood supply, the dentin can become more brittle over time, making the tooth more susceptible to fracture. The aforementioned discoloration is also a common cosmetic concern. This is why teeth that have undergone root canal treatment (a procedure to remove necrotic pulp and disinfect the canals) are often recommended to have a crown placed on them to provide structural support and protection.
The Body’s Continuous Battle
It’s important to remember that even with chronic, low-grade infections where symptoms are minimal, the body is still fighting. Immune cells are constantly being recruited to the area to try and contain the bacteria. This can lead to the formation of granulation tissue, a type of inflammatory tissue rich in blood vessels and immune cells, at the root tip. Sometimes this can encapsulate the infection, forming a periapical granuloma. While this might keep the infection localized for a time, it’s not a cure, and the potential for a flare-up (acute exacerbation) always exists if the bacterial load increases or the body’s defenses are weakened.
Early Detection is Key
Understanding what happens inside the pulp when a tooth is damaged highlights the critical importance of regular dental check-ups and prompt attention to any dental symptoms. When problems like decay are caught early, they can often be treated simply, preventing the cascade of events that leads to pulpitis, necrosis, and periapical infection. Listening to your teeth when they whisper with mild sensitivity can save you from hearing them scream in pain later on, and it can preserve the vitality and longevity of these essential structures.
The journey from a healthy pulp to a necrotic, infected space is a complex biological process driven by the tooth’s reaction to injury and the subsequent bacterial invasion. It underscores the delicate balance within our oral environment and the serious consequences that can arise when that balance is disrupted by damage or disease.