The intricate network of nerves supplying our teeth and their supporting structures, known as periodontal tissues, is a marvel of biological engineering. This system is not just about feeling pain; it’s a sophisticated sensory apparatus that provides a wealth of information to our brain, influencing everything from how we chew to protecting our oral cavity from harm. Understanding this innervation sheds light on the various sensations we experience in our mouths, from the sharp twinge of a sensitive tooth to the subtle pressures of biting into an apple.
The Master Conductor: The Trigeminal Nerve
The primary source of sensory innervation to the teeth and periodontal tissues is the trigeminal nerve, also known as the fifth cranial nerve (CN V). This is the largest cranial nerve and it branches out extensively to cover most of the face, including the oral cavity. It’s a mixed nerve, meaning it has both sensory and motor functions, but for our discussion on tooth and periodontal sensation, we are primarily interested in its sensory components.
Key Branches for Oral Innervation
The trigeminal nerve splits into three main divisions, and two of these are crucial for oral structures:
The maxillary nerve (V2) is the second division. After exiting the skull, it gives rise to several branches that supply the upper teeth, the maxillary sinus, the palate, and parts of the nasal cavity and mid-face. Specifically for the upper teeth and their surrounding periodontium, branches like the posterior superior alveolar (PSA) nerve, middle superior alveolar (MSA) nerve, and anterior superior alveolar (ASA) nerve are paramount. These nerves form a plexus, or network, above the roots of the maxillary teeth, sending delicate fibers into each tooth and the adjacent periodontal tissues.
The mandibular nerve (V3) is the third and largest division. It’s unique among the trigeminal divisions as it carries both sensory and motor fibers (the motor fibers control the muscles of mastication). For dental innervation, its most significant sensory branch is the inferior alveolar nerve (IAN). The IAN travels within the mandible, giving off branches to all the lower teeth and their supporting structures before emerging near the chin as the mental nerve (supplying the chin and lower lip). Other branches of the mandibular nerve, like the lingual nerve (sensation to the anterior two-thirds of the tongue and floor of the mouth) and the buccal nerve (sensation to the cheek and buccal gingiva of the mandibular molars), also contribute to the overall sensory picture of the lower oral cavity.
Journey Inside the Tooth: Pulp Innervation
The dental pulp, the soft living tissue at the core of each tooth, is richly innervated. Nerve fibers, typically bundled with blood vessels, enter the tooth through a tiny opening at the tip of the root called the apical foramen. Once inside the pulp chamber and root canals, these nerve bundles branch extensively, forming a dense network, especially in the coronal pulp (the part within the crown of the tooth) just beneath the dentin layer. This is known as the plexus of Raschkow.
Several types of nerve fibers are found within the pulp:
- A-delta (Aδ) fibers: These are thinly myelinated sensory fibers. They are primarily responsible for the sharp, well-localized pain often associated with dentinal hypersensitivity or initial pulpitis. They have a relatively low stimulation threshold.
- C-fibers: These are unmyelinated sensory fibers, more numerous than A-delta fibers. They are associated with dull, throbbing, or radiating pain, often indicative of more advanced pulpal inflammation. C-fibers have a higher stimulation threshold but can produce more intense and lingering pain.
- Sympathetic fibers: These are autonomic nerve fibers that travel with the blood vessels. Their primary role is vasomotor, meaning they regulate blood flow within the pulp by causing constriction of the arterioles. They are not directly involved in pain sensation but can influence the pulpal environment.
Sensory Perception from the Pulp
The overwhelming sensation perceived from direct stimulation of the dental pulp is pain (nociception). While there’s some debate, the pulp is generally not considered to possess true mechanoreceptors for light touch or proprioceptors for position sense in the same way the periodontal ligament does. Stimuli like temperature changes (hot or cold), pressure, or tissue damage within the pulp are typically interpreted as pain. This is why it can be difficult to pinpoint the exact tooth causing pulpal pain, especially in its early stages; the pain often feels diffuse.
One widely accepted explanation for how stimuli applied to the outer dentin surface (like cold air or sweets) can cause sharp pain is the hydrodynamic theory. This theory suggests that such stimuli cause a rapid movement of fluid within the microscopic dentinal tubules (tiny channels running through the dentin). This fluid movement is thought to distort mechanosensitive A-delta nerve endings located near the pulp-dentin border or extending slightly into the tubules, triggering a pain signal.
Supporting Structures: Periodontal Tissue Innervation
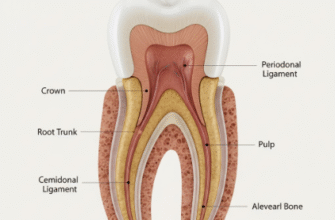
The periodontium comprises the tissues that surround and support the teeth: the gingiva (gums), the periodontal ligament (PDL), the alveolar bone (tooth socket), and the cementum (covering the tooth root). These tissues are also extensively innervated, providing a different spectrum of sensory information compared to the pulp.
The Periodontal Ligament (PDL): A Sensory Hub
The periodontal ligament (PDL) is a fibrous connective tissue that anchors the tooth root to the alveolar bone. It is exceptionally rich in sensory nerve fibers, making it a critical structure for oral sensation and function. Unlike the pulp, which primarily signals pain, the PDL can discriminate various mechanical stimuli:
- Proprioception: This is the sense of position and movement. PDL mechanoreceptors provide precise feedback about tooth position, contact with opposing teeth, and the forces applied during biting and chewing. This information is vital for the fine control of masticatory muscles.
- Touch and Pressure: The PDL allows us to perceive very light touch on a tooth (e.g., a single hair) and to gauge the texture and hardness of food.
- Pain (Nociception): The PDL also contains nociceptors that signal pain in response to excessive forces, inflammation (as in periodontal disease), or trauma. Pain originating from the PDL is usually well-localized to the specific tooth involved.
Various types of specialized nerve endings are found in the PDL, including Ruffini-like endings (sensitive to sustained pressure and stretch), as well as unmyelinated free nerve endings (often associated with pain and temperature). This diverse array of receptors contributes to the PDL’s sophisticated sensory capabilities, playing a crucial role in reflexes like the jaw-opening reflex, which protects teeth from excessive biting forces.
The rich and diverse innervation of the periodontal ligament allows for precise localization of stimuli applied to a tooth, such as pressure or touch. This contrasts sharply with the more diffuse and often poorly localized pain originating from the dental pulp. This functional difference is critical for how our brain interprets various oral sensations and protects the dental structures.
Gingival Innervation
The gingiva, or gums, is also well-supplied with sensory nerves. These nerves are branches from the same larger nerves that supply the teeth and alveolar bone, such as the superior alveolar nerves for the upper gingiva and branches of the inferior alveolar, lingual, and buccal nerves for the lower gingiva. The gingiva contains receptors for touch, pressure, temperature, and pain. This allows us to sense food texture against the gums, detect temperature variations, and perceive pain from injuries or inflammation like gingivitis.
Alveolar Bone and Cementum Innervation
The alveolar bone that forms the tooth sockets receives some sensory and autonomic innervation, primarily associated with its periosteum (the outer membrane covering the bone) and its vascular supply. While not as densely innervated for fine sensation as the PDL, it can be a source of pain, especially during inflammatory processes or trauma.
Cementum, the hard tissue covering the tooth root, is generally considered acellular (in its acellular variant) and aneural. Its primary role is to provide attachment for the PDL fibers. Sensory perception related to the root surface usually originates from the adjacent PDL or, if root exposure occurs, from the underlying dentin.
The Autonomic Nervous System’s Subtle Role
Beyond the dominant sensory innervation, the autonomic nervous system (ANS), specifically sympathetic fibers, also plays a role in the oral cavity. These sympathetic nerves typically travel along with blood vessels. Their primary function in both the dental pulp and the periodontal tissues is vasomotor control – regulating blood vessel diameter and thus blood flow. By causing vasoconstriction (narrowing of blood vessels), they can modulate blood supply to these tissues.
While not directly generating sensations like pain or touch, the ANS can influence the local tissue environment. For instance, changes in blood flow can affect nutrient supply, waste removal, and the inflammatory response in both the pulp and periodontium. There is ongoing research into how autonomic activity might modulate immune responses and healing processes in these tissues, highlighting a more complex interaction than previously understood.
In summary, the innervation of teeth and periodontal tissues is a complex and highly specialized system. From the sharp pain signals relayed by pulpal nerves to the nuanced information about pressure and position provided by the periodontal ligament, this neural network is essential for normal oral function, protection against damage, and the rich tapestry of sensations we experience when we eat, speak, and interact with our environment through our mouths. Understanding this intricate system underscores the delicate balance required for oral health and comfort.