The Hidden Life Within Your Tooth: An Introduction to Dental Pulp
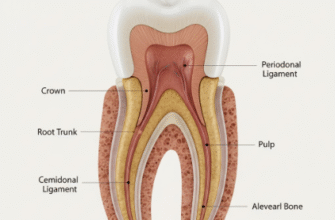
Deep inside every tooth, beneath the hard outer layers of enamel and dentin, lies a soft, vital core known as the dental pulp. Often referred to as the “nerve” of the tooth, it’s much more than just that. This remarkable tissue is a complex mix of living cells, blood vessels, nerves, and connective tissue. Think of it as the tooth’s control center and life support system, housed within a rigid chamber.
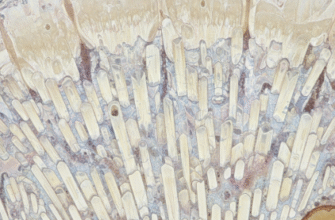
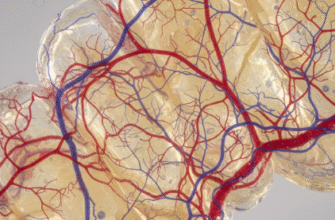
Key components include odontoblasts, specialized cells lining the pulp-dentin border, responsible for producing dentin throughout life. Blood vessels provide essential nutrients and oxygen, while nerves transmit sensations like pain, temperature, and pressure. Lymphatic vessels also play a role in fluid balance and immune responses. The pulp’s primary jobs include forming dentin (both initially and in response to wear or injury), providing sensation, and mounting a defense against threats.
When Trouble Knocks: Common Irritants to the Dental Pulp
The dental pulp, despite its protected location, is constantly under potential threat from various sources. Understanding these irritants is the first step in appreciating how the pulp responds to maintain tooth health.
Bacterial Invasion: The Usual Suspect
By far the most common irritant is bacteria, primarily from dental caries (cavities). As bacteria break down tooth structure, they produce toxins and byproducts that seep through the microscopic channels in dentin, called dentinal tubules, eventually reaching the pulp. Periodontal disease, if it progresses deep enough to reach the tooth’s apex (root tip), can also introduce bacteria directly into the pulp.
Mechanical and Traumatic Forces
Physical forces can also upset the pulp’s delicate balance. This includes:
- Dental Procedures: Deep fillings, crown preparations, or even the heat generated by drilling can irritate the pulp. The closer the procedure gets to the pulp, the higher the risk.
- Trauma: A knock or blow to a tooth can cause direct injury, sometimes leading to inflammation or even severing the blood supply.
- Bruxism: Chronic teeth grinding or clenching puts excessive force on teeth, potentially leading to micro-cracks and pulp irritation over time.
- Orthodontic Movement: While generally safe, rapid or excessive tooth movement during orthodontic treatment can sometimes cause transient pulpal inflammation.
Chemical Challenges
Certain chemicals can also act as irritants. Acidic foods and drinks, if consumed frequently, can erode enamel and expose dentin, making the pulp more vulnerable. Some dental restorative materials, if not placed with care or if they leach components, can cause a chemical irritation. Even some tooth-whitening agents, if used improperly or in excessive concentrations, can lead to temporary sensitivity, indicating mild pulpal irritation.
Thermal Shocks
Sudden or extreme temperature changes can stimulate the pulp. Think of the sharp sensation when biting into ice cream or sipping hot coffee. While often transient, prolonged exposure or very large metallic restorations (which conduct temperature changes rapidly) can lead to more persistent irritation.
Sounding the Alarm: The Pulp’s Initial Defense Mechanisms
When faced with an irritant, the dental pulp doesn’t just passively succumb. It has a sophisticated set of defense mechanisms designed to protect itself and the tooth. The nature and intensity of the irritation largely dictate the type and extent of this response.
One of the earliest reactions can be an increased outward flow of dentinal fluid within the tubules. This is thought to help flush out irritants and slow their inward progression. More significantly, the odontoblasts, those specialized cells at the pulp-dentin border, spring into action.
Wall Building: Reactionary and Reparative Dentin
If the irritation is mild and the odontoblasts survive the initial insult, they can be stimulated to produce reactionary dentin. This is essentially an extra layer of dentin laid down on the pulpal side of the existing dentin, thickening the barrier between the pulp and the irritant. It’s a slower, more organized process.
However, if the irritation is more severe and some odontoblasts are damaged or die, a different process kicks in. Undifferentiated mesenchymal cells within the pulp can be signaled to migrate to the injury site, differentiate into new odontoblast-like cells, and then lay down a layer of reparative dentin. This type of dentin is often less organized than reactionary dentin but serves the same crucial purpose: to wall off the pulp from the offending agent. The formation of reparative dentin is a clear sign that the pulp is actively fighting back against a more significant threat.
The Inflammatory Cascade
Simultaneously, the pulp initiates an inflammatory response, much like any other connective tissue in the body when injured. This involves:
- Vasodilation: Blood vessels within the pulp widen, increasing blood flow to the area. This brings more defensive cells and nutrients.
- Increased Vascular Permeability: The walls of these blood vessels become more porous, allowing plasma fluid and immune cells to leak out into the surrounding pulp tissue. This can lead to increased pressure within the confined pulp chamber.
- Release of Mediators: Various chemical messengers, such as cytokines, prostaglandins, and neuropeptides, are released. These orchestrate the inflammatory response, attracting immune cells and also sensitizing nerve fibers, which often translates to pain.
- Recruitment of Immune Cells: Neutrophils are typically the first responders, followed by macrophages, lymphocytes, and plasma cells, all working to neutralize bacteria, clear debris, and manage the injury.
This inflammatory response, while protective, is a double-edged sword. The pulp is encased in a rigid, unyielding dentin shell. Swelling, a hallmark of inflammation elsewhere in the body, cannot easily occur. Instead, the increased fluid and cellular influx can dramatically raise the intrapulpal pressure, compressing blood vessels and nerve fibers, potentially leading to further damage and intense pain.
From Mild Discomfort to Serious Trouble: Stages of Pulp Response
The interaction between irritants and the pulp’s defense mechanisms can lead to a spectrum of conditions collectively known as pulpitis, or inflammation of the pulp. The progression and outcome depend heavily on the severity and duration of the irritation, as well as the pulp’s ability to cope.
Reversible Pulpitis: A Chance for Recovery
When the irritation is mild and transient, the pulp may experience what’s termed reversible pulpitis. In this stage, the inflammation is slight, and the pulp tissue has the capacity to heal fully if the source of irritation is identified and removed promptly. For example, removing a shallow carious lesion and placing a well-sealed filling can allow the pulp to return to a healthy state.
Symptoms often include a sharp, short-lived pain, typically elicited by stimuli like cold, sweet, or sometimes air. The pain subsides quickly, within seconds of the stimulus being removed. There’s usually no spontaneous pain (pain occurring without an obvious trigger).
Persistent or severe irritation to the dental pulp can lead to irreversible damage and eventual tissue death.
Ignoring symptoms like prolonged tooth sensitivity or spontaneous pain can result in more complex and costly treatments.
Early detection and intervention are crucial for preserving pulp vitality.
Irreversible Pulpitis: Past the Point of No Return
If the irritation is more severe, prolonged, or if the pulp’s defenses are overwhelmed, the condition can progress to irreversible pulpitis. At this stage, the inflammatory changes within the pulp are so significant that the tissue cannot recover, even if the original irritant is removed. The pulp is destined to die.
Symptoms can vary but often include more intense and prolonged pain. The pain might be spontaneous, waking a person at night. It can be a dull, throbbing ache or a sharp, lingering pain. Heat often exacerbates the pain, while cold might provide temporary relief in some instances (as it can cause vasoconstriction, momentarily reducing intrapulpal pressure). The pain can also be difficult to localize, sometimes feeling like it’s coming from adjacent teeth or even other areas of the face (referred pain).
It’s important to note that irreversible pulpitis can sometimes be asymptomatic, meaning it progresses silently without causing noticeable pain, especially in cases of slow, chronic irritation. The pulp is still dying, but the process is more insidious.
Pulp Necrosis: The End of Vitality
Untreated irreversible pulpitis invariably leads to pulp necrosis, which is the death of the pulp tissue. The once-vital inner core of the tooth becomes a lifeless, often infected space. A tooth with a necrotic pulp may initially become asymptomatic as the nerve fibers die. However, it can also be tender to touch or biting (percussion sensitivity), especially if the inflammatory process starts to affect the tissues surrounding the root tip (the periapical area).
Once the pulp is necrotic, it can no longer defend itself. Bacteria can freely proliferate within the root canal system. This can lead to the infection spreading beyond the tooth’s apex, causing a periapical abscess or chronic inflammation in the bone around the root tip (apical periodontitis). This highlights why addressing pulpal issues before they reach necrosis is so important.
The Tipping Point: Factors Influencing the Pulp’s Fate
The dental pulp’s journey from health to disease isn’t always straightforward. Several factors can influence how it responds to an irritant and whether that response will be successful in preserving its vitality.
The Irritant’s Profile
The nature, intensity, and duration of the irritant are paramount. A mild, short-lived irritant (like slight heat from polishing a filling) is far less likely to cause lasting damage than a deep carious lesion teeming with bacteria that has been present for months. The virulence of the specific bacteria involved in caries also plays a role.
Host Factors: The Individual’s Role
The patient’s overall health and age can impact pulpal response. Younger pulps generally have a better blood supply and more cellular vitality, giving them a greater capacity for repair. Conversely, older pulps may have reduced vascularity and cellularity, and more fibrous tissue, potentially compromising their healing ability. Systemic conditions that affect blood flow or immune function could also theoretically influence pulpal healing, though the direct impact is complex and still being researched.
The Protective Barrier: Remaining Dentin Thickness (RDT)
The amount of healthy dentin between the floor of a cavity preparation (or the source of irritation) and the pulp is a critical factor. This is known as the Remaining Dentin Thickness (RDT). A thicker layer of dentin provides better insulation and protection for the pulp. Dental procedures that significantly reduce RDT, bringing the operative site very close to the pulp, carry a higher risk of inducing irreversible pulpal changes. Even the permeability of the dentin itself, which can vary, influences how quickly irritants can reach the pulp.
Pathways for Invasion
The presence of direct pathways for irritants to access the pulp dramatically increases risk. Open dentinal tubules (exposed by caries, wear, or aggressive tooth preparation), cracks in the tooth that extend towards the pulp, or leaking dental restorations can all provide easy avenues for bacteria and their toxins to penetrate and cause inflammation.
The Aftermath: Long-Term Consequences of Chronic Pulp Irritation
If pulpal irritation isn’t addressed or if the pulp undergoes chronic, low-grade inflammation, several long-term changes can occur within the tooth, even if it doesn’t immediately progress to symptomatic irreversible pulpitis or necrosis.
Pulp Calcification: Hardening from Within
One common response to chronic irritation is the formation of calcifications within the pulp chamber and root canals. These can be diffuse, spread throughout the pulp tissue, or they can form discrete masses known as pulp stones (denticles). While often an incidental finding on radiographs and not necessarily problematic in themselves, extensive calcification can make future root canal treatment, if needed, more challenging by obstructing access to the canals.
Internal Resorption: A Rare but Destructive Process
Less commonly, chronic inflammation can trigger cells within the pulp (odontoclasts) to start resorbing the dentin from the inside out. This is known as internal resorption. It can appear as a pinkish spot on the tooth if it erodes through to the enamel, or as an irregular enlargement of the pulp space on an X-ray. If left untreated, internal resorption can weaken the tooth structure significantly, potentially leading to fracture.
The Inevitable Slide to Necrosis and Beyond
Ultimately, most forms of chronic, unresolved pulp inflammation will eventually lead to pulp necrosis. As discussed earlier, a necrotic pulp is a haven for bacteria, and the infection will almost invariably spread beyond the root tip, leading to periapical periodontitis. This can manifest as a painful dental abscess (an acute flare-up) or a chronic, often asymptomatic, lesion visible on an X-ray at the root end. These conditions require root canal treatment or extraction to resolve the infection and prevent further complications.
The Bigger Picture: Why Understanding Pulp Response is Vital
Grasping the intricacies of how the dental pulp reacts to irritation is not just an academic exercise. It has profound implications for both dental professionals and patients. For dentists, this knowledge underpins diagnostic processes, helping to differentiate between reversible and irreversible conditions. It guides treatment planning, aiming to preserve tooth vitality whenever possible through conservative interventions, or opting for root canal therapy when the pulp is beyond saving.
For individuals, understanding that even minor tooth decay or a small chip can initiate a cascade of events within the pulp underscores the importance of regular dental check-ups and early intervention. Recognizing early warning signs, like sensitivity to cold or sweets, and seeking prompt dental care can often mean the difference between a simple filling and a more complex procedure. Ultimately, a healthy pulp means a healthy, functional tooth, contributing to overall well-being.