Ever wondered what keeps your teeth firmly in place, allowing you to bite into a crunchy apple or chew a hearty meal? It’s not just the tooth itself, but a sophisticated support system working tirelessly behind the scenes. This intricate network of tissues is collectively known as the periodontium, a term derived from Greek words: “peri” meaning around, and “odont” meaning tooth. Essentially, it’s everything that surrounds and supports your teeth, anchoring them within the jawbones and acting as a crucial barrier against the bustling environment of your mouth.
Understanding the structure of the periodontium is like appreciating the foundation of a house; without a strong and healthy foundation, the house cannot stand tall. Similarly, the health and stability of our teeth are directly dependent on the integrity of these supporting tissues. Let’s delve into the fascinating architecture of this vital system.
The Four Pillars of Tooth Support
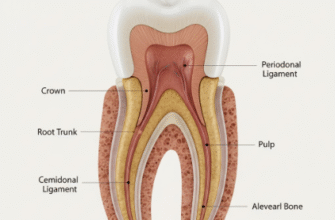
The periodontium isn’t a single entity but rather a complex made up of four distinct, yet interconnected, tissues. Each plays a unique role, contributing to the overall function of supporting the teeth and maintaining their position. These four key players are:
- The Gingiva (commonly known as gums)
- The Periodontal Ligament (PDL)
- The Cementum (covering the tooth root)
- The Alveolar Bone (the jawbone that houses the teeth)
Imagine these components working in concert: the gingiva provides a protective seal, the alveolar bone forms the socket, the cementum lines the root, and the periodontal ligament acts as the flexible sling connecting the tooth to the bone, cushioning it against forces.
The Gingiva: The First Line of Defense
The gingiva, or gums, is the soft, pink tissue you see surrounding the necks of your teeth. It’s the most visible part of the periodontium and plays a critical role in protecting the underlying tissues from mechanical trauma and bacterial invasion from the oral cavity. It’s like a tight collar around each tooth.
The gingiva is specialized oral mucosa and can be further divided into several distinct anatomical areas:
Free Gingiva
This is the unattached, coronal portion of the gingiva that forms the soft tissue wall of the gingival sulcus – a shallow crevice or groove between the tooth and the gum. Think of it as a tiny moat around the tooth. Its edge, the gingival margin, is typically knife-edged in health.
Attached Gingiva
Continuous with the free gingiva, the attached gingiva is firmly bound to the underlying periosteum of the alveolar bone and to the cementum by connective tissue fibers. It’s stippled, resembling the surface of an orange peel, which is a sign of health. This firm attachment is crucial for providing stability and withstanding the frictional stresses of chewing.
Interdental Gingiva (Papilla)
This is the portion of the gingiva that occupies the space between two adjacent teeth, just below their contact point. In the front of the mouth, it’s often pyramidal in shape, while in the back, it’s more flattened, forming a “col” shape that conforms to the space between the molars. The interdental papilla prevents food from being wedged between teeth.
Microscopically, the gingiva consists of a core of connective tissue covered by stratified squamous epithelium. The epithelium facing the oral cavity is keratinized, providing a tough, protective surface, while the epithelium lining the sulcus (sulcular epithelium) and facing the tooth (junctional epithelium) is non-keratinized. The junctional epithelium is particularly important as it forms a seal between the gingiva and the tooth surface, a critical defense mechanism.
The Periodontal Ligament: The Tooth’s Suspension System
Nestled between the tooth root and the alveolar bone is the periodontal ligament, or PDL. This is not a simple ligament in the way you might think of one joining bones in a joint; instead, it’s a highly specialized and dynamic connective tissue, a sort of fibrous sling that suspends the tooth within its socket. It’s remarkably thin, typically ranging from 0.15 to 0.38 millimeters in width, yet incredibly strong and complex.
The PDL is primarily composed of organized collagen fiber bundles, known as Sharpey’s fibers, which embed into the cementum of the tooth root on one side and the alveolar bone on the other. These fibers are not static; they are constantly being remodeled and adapted to the forces placed on the teeth.
Principal Fibers of the PDL
The principal fibers are organized into distinct groups, named according to their location and orientation. These groups include:
- Alveolar Crest Fibers: Run from the cementum just below the junctional epithelium to the alveolar crest. They resist tilting, intrusive, extrusive, and rotational forces.
- Horizontal Fibers: Extend at right angles to the long axis of the tooth, from cementum to alveolar bone. They resist horizontal and tilting forces.
- Oblique Fibers: The most numerous group, running obliquely from the cementum to the bone in a coronal direction. They bear the brunt of vertical chewing forces, suspending the tooth in the socket.
- Apical Fibers: Radiate from the cementum around the apex of the root to the bone, forming the base of the socket. They prevent tooth tipping and dislocation, and protect blood vessels and nerves entering the tooth.
- Interradicular Fibers (in multi-rooted teeth): Found in the furcations (between the roots) of multi-rooted teeth, fanning out from cementum to the interradicular bone. They help stabilize the tooth.
Beyond these structural fibers, the PDL is a bustling hub of cellular activity. It contains fibroblasts (which produce and maintain the fibers and ground substance), osteoblasts and osteoclasts (for bone formation and resorption), cementoblasts (for cementum formation), and undifferentiated mesenchymal cells. It also has a rich supply of blood vessels providing nutrition, and an extensive nerve supply that provides a highly sensitive sense of touch, pressure, and pain, allowing us to detect even the smallest particle between our teeth.
The functions of the PDL are manifold:
- Supportive: Attaches the tooth to the bone and maintains it in the socket.
- Shock Absorption: Cushions the tooth and bone against occlusal forces.
- Formative and Remodeling: Cells in the PDL participate in the formation and resorption of cementum and bone, allowing for tooth movement and adaptation.
- Nutritive: Blood vessels provide nutrients to the cementum, bone, and gingiva.
- Sensory: Nerves provide proprioception (sense of position) and pain sensation.
The periodontal ligament is a truly remarkable tissue. It not only anchors the tooth but also acts as a shock absorber, distributing chewing forces to the bone. Its rich nerve supply provides vital sensory feedback, and its cells are crucial for maintaining and repairing the surrounding tissues throughout life.
Cementum: The Root’s Protective Coat
Cementum is the hard, calcified tissue that covers the anatomical root of the tooth. It’s a bone-like substance, but it’s avascular (lacks blood vessels) and has no nerve supply, making it less sensitive than dentin. Its primary role is to provide a surface for the attachment of the periodontal ligament fibers, thus anchoring the tooth.
Cementum is typically yellowish in color and softer than dentin and enamel. It starts at the cementoenamel junction (CEJ), where the enamel covering the crown ends and the cementum begins. The nature of this junction can vary: sometimes cementum overlaps enamel, sometimes they meet end-to-end, and sometimes there’s a small gap exposing dentin.
Types of Cementum
There are two main types of cementum, based on the presence or absence of cells (cementocytes) within its matrix:
- Acellular Cementum (Primary Cementum): This forms first and covers the cervical third or half of the root, closest to the crown. It’s thinner and forms before the tooth erupts. It plays a major role in tooth anchorage, as the principal fibers of the PDL (Sharpey’s fibers) are embedded directly into it.
- Cellular Cementum (Secondary Cementum): This is formed after tooth eruption and is found mainly on the apical third of the root and in interradicular areas. It is thicker and contains cementocytes, which are cells trapped within the cementum matrix, residing in spaces called lacunae. Cellular cementum is laid down throughout life in response to functional demands and wear, helping to compensate for occlusal wear by continuous deposition at the apex.
Cementum is not a static tissue. It can undergo resorption (removal) by cells called odontoclasts, similar to bone resorption. However, it also has a reparative capacity, with new cementum being deposited by cementoblasts. This dynamic nature allows the tooth to adapt to changing occlusal forces and to repair minor root damage.
Alveolar Bone: The Jaw’s Embrace
The alveolar bone, also known as the alveolar process, is the specialized part of the maxilla (upper jaw) and mandible (lower jaw) that forms the sockets and supports the teeth. It develops with the teeth and is resorbed if teeth are lost, highlighting its dependence on their presence.
The wall of the tooth socket (alveolus) is composed of several types of bone:
Alveolar Bone Proper (Cribriform Plate or Lamina Dura)
This is a thin layer of compact bone that directly lines the tooth socket. It’s called the cribriform plate because it’s perforated by numerous small openings (Volkmann’s canals) through which blood vessels, lymphatics, and nerves pass between the PDL and the bone. Radiographically, it appears as a dense white line called the lamina dura, and its integrity is an important indicator of periodontal health.
Cortical Bone
This forms the hard, outer wall of the alveolar process on the facial (cheek/lip) and lingual (tongue) sides. It’s dense and provides structural support. The thickness of cortical bone varies in different parts of the mouth.
Cancellous Bone (Spongy Bone)
Located between the alveolar bone proper and the cortical plates, cancellous bone consists of a network of bony trabeculae enclosing marrow spaces. It provides support and acts as a reservoir for minerals. The arrangement of trabeculae often reflects the stress patterns placed on the bone.
The alveolar bone is a highly dynamic tissue, constantly undergoing remodeling (formation and resorption) in response to functional demands, such as chewing forces and tooth movement (like during orthodontic treatment). Osteoblasts are responsible for bone formation, while osteoclasts are responsible for bone resorption. This plasticity allows the teeth to adapt to changes in occlusion and to move through the bone.
A Symphony of Support
No single component of the periodontium works in isolation. The gingiva provides the initial protective seal. The cementum on the root surface provides the attachment for the periodontal ligament fibers. These fibers, in turn, embed into the alveolar bone proper, suspending the tooth in its socket. The bulk of the alveolar bone then supports this entire apparatus.
The blood supply and nerve innervation are also shared and integrated, ensuring that the entire system functions cohesively. When you chew, the forces are transmitted from the tooth, through the PDL, to the alveolar bone. The PDL’s unique structure dissipates these forces, preventing damage to the tooth and bone. This intricate interplay is what allows our teeth to withstand the significant forces of mastication day in and day out, for many years.
Maintaining the health of these supporting structures is paramount for long-term tooth retention and overall oral comfort. A well-functioning periodontium not only keeps teeth stable but also contributes to the aesthetics of a smile and the ability to speak and eat properly. It truly is a marvel of biological engineering, perfectly designed for its crucial role.