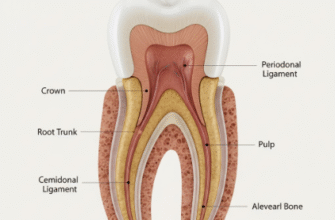
The periodontal ligament, often abbreviated as PDL, is a truly remarkable connective tissue. It’s the vital link, the flexible sling, that anchors our teeth firmly within their bony sockets in the jaw. Think of it as a highly specialized suspension system, constantly working to withstand the immense forces generated during chewing, talking, and even just clenching. At the heart of this system’s strength and resilience lies an intricate network of protein fibers, and among these, collagen reigns supreme. Understanding the different types of collagen fibers within the PDL is like deciphering the blueprint of this biological marvel, revealing how our teeth are so effectively supported yet capable of slight, essential movement.
Collagen, in a broader sense, is the most abundant protein in mammals, making up a significant portion of our skin, bones, tendons, and ligaments. It’s the body’s primary structural protein, providing tensile strength – that ability to resist being pulled apart. Imagine a rope; collagen fibers act much like the individual strands woven together to give the rope its toughness. These fibers are not just inert scaffolding, though. They are dynamic structures, constantly being remodeled and replaced, especially in active tissues like the PDL, allowing for adaptation and repair.
The Collagen Cast: Key Players in the PDL
The PDL is not just a homogenous band of tissue; it’s a sophisticated matrix where different collagen types collaborate to achieve its unique functional properties. Each type brings distinct characteristics to the table, contributing to the overall performance of this critical dental structure.
Type I Collagen: The Backbone of Support
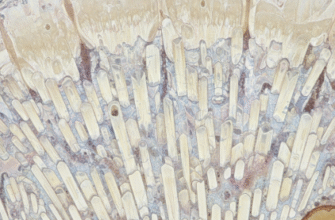
When we talk about the PDL’s structural integrity, Type I collagen is undoubtedly the star of the show. It constitutes the vast majority, typically around 70-80%, of the collagen found in this ligament. These are thick, robust fibers, forming the principal fiber bundles – often called Sharpey’s fibers when they embed into cementum (the tooth root surface) and alveolar bone. Their primary role is to provide immense tensile strength, allowing the tooth to resist displacement forces from various directions. Whether you’re biting into a crunchy apple or grinding your teeth unconsciously, Type I collagen is working hard to keep things stable. These fibers are meticulously organized into distinct groups based on their orientation (such as alveolar crest, horizontal, oblique, apical, and interradicular fibers), each designed to counteract specific forces and support the tooth during function. The oblique fibers, for instance, are the most numerous and play a key role in suspending the tooth and translating masticatory pressures into tension on the alveolar bone.
Type III Collagen: The Reticular Reinforcer
Working in close association with Type I collagen is Type III collagen, often referred to as reticular fibers due to the fine, delicate network they form. While not as bulky or as strong individually as Type I fibers, Type III plays a crucial role in the PDL’s overall architecture and elasticity. It’s particularly abundant during development and wound healing, acting as a sort of temporary scaffold before more robust Type I fibers are laid down. In the mature PDL, Type III collagen contributes to the suppleness of the tissue, allowing for slight, controlled tooth movement, which is essential for distributing occlusal forces effectively and preventing damage. It’s often found co-mingled with Type I within the same fibrils, suggesting a synergistic relationship where Type III might influence the organization, diameter, and overall biomechanical properties of the larger Type I fibers. Think of it as the finer threads that add flexibility and resilience to a predominantly strong fabric, ensuring the ligament isn’t too rigid.
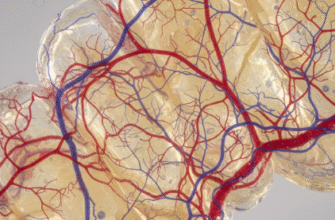
The periodontal ligament is a highly vascular and cellular connective tissue. Beyond collagen fibers, it contains a rich mix of cells like fibroblasts, osteoblasts, osteoclasts, cementoblasts, and epithelial cell rests of Malassez. This cellular diversity underscores its dynamic role in tooth support, maintenance, and repair processes.
Type V Collagen: The Fibril Diameter Regulator
Delving deeper into the microscopic organization, we encounter Type V collagen. This type is present in much smaller quantities compared to Type I and III, but its function is disproportionately important for the correct formation of the ligament’s architecture. Type V collagen is intimately associated with Type I collagen fibrils, often found within the core of these larger fibrils or on their surface. Its primary role is believed to be in regulating the diameter of these Type I fibrils during their formation (fibrillogenesis). By controlling fibril size, Type V collagen influences the overall mechanical properties of the ligament, such as its tensile strength and elasticity. If Type I fibrils were all of varying, uncontrolled thicknesses, the ligament wouldn’t perform as predictably or efficiently. So, Type V acts as a subtle but critical quality control manager, ensuring the building blocks (the Type I fibrils) are formed correctly for optimal function and uniform strength. Its presence is vital for the proper assembly and stability of the collagenous network, preventing the formation of excessively large or irregular fibrils.
Type VI Collagen: The Anchoring Microfibrillar Network
Moving beyond the classic fibrillar collagens that form long, banded structures, we find Type VI collagen. This fascinating collagen doesn’t form the large, banded fibrils typical of Type I or III. Instead, Type VI assembles into a unique beaded microfibrillar network that permeates the extracellular matrix of the PDL, surrounding other collagen fibers, cells, and blood vessels. Its function is multifaceted and distinct. Type VI collagen plays a role in cell adhesion, helping to connect cells, particularly fibroblasts, to the surrounding matrix, thus influencing cell behavior and matrix organization. It also contributes to the structural integrity of the tissue by linking larger collagen bundles and other matrix components, like proteoglycans, together. Think of it as a fine, pervasive mesh that helps to hold everything in its proper place and maintain the overall organization and cohesion of the ligament. It’s also thought to provide a degree of elasticity and flexibility to the tissue at a micro-level, acting as a sort of shock absorber and protecting cells from mechanical stress.
Type XII Collagen: The Interfacer and Organizer
Another interesting player in the PDL’s collagen story is Type XII collagen. This is a member of the FACIT (Fibril Associated Collagens with Interrupted Triple helices) family. As the name suggests, FACIT collagens don’t form fibrils themselves but rather associate with the surface of existing fibrils, particularly Type I collagen fibrils. Type XII collagen, with its large, non-collagenous N-terminal domain that projects outwards from the fibril surface, is thought to mediate interactions between Type I collagen fibrils and other extracellular matrix components or even cells. This suggests a role in organizing the collagenous matrix, maintaining appropriate spacing between the fibrils, and potentially influencing the tissue’s response to mechanical stress by modulating the slippage between fibrils. It’s like a specialized connector or spacer, ensuring that the main structural fibers are properly integrated into the broader matrix environment and can interact effectively with their surroundings. Its presence highlights the complexity and fine-tuning involved in creating a functional periodontal ligament capable of adapting to various loads.
A Dynamic and Cohesive System
It’s crucial to remember that the collagen network in the periodontal ligament is not a static structure. It’s a highly dynamic environment, with a relatively high rate of turnover compared to other connective tissues like tendons. Fibroblasts, the primary cells within the PDL, are constantly synthesizing new collagen molecules and, with the help of enzymes like collagenases, breaking down old or damaged ones. This continuous remodeling process allows the PDL to adapt to changing functional demands, such as alterations in bite forces, repair micro-damage incurred during normal function, and maintain its integrity throughout life. The various types of collagen don’t work in isolation. Instead, they form a complex, interconnected system where each type fulfills specific roles that contribute to the ligament’s overall function.
The immense strength of Type I, the flexibility and developmental support imparted by Type III, the fibril regulatory role of Type V, the anchoring and cell-interactive function of Type VI, and the organizational influence of Type XII all contribute synergistically to the unique properties of the periodontal ligament. This sophisticated interplay ensures that our teeth can withstand the daily rigors of mastication, providing stable yet flexible support. The precise balance and interaction between these different collagen types are fundamental to oral health, enabling the PDL to perform its critical shock-absorbing, supportive, and sensory functions effectively, distributing forces and protecting both the tooth and the surrounding alveolar bone from injury.