Ever wondered how that ice cream sends a jolt through your molar, or how you can tell exactly where that tiny popcorn kernel is stuck? The answer lies in a remarkably intricate network of nerves dedicated to providing sensation to your teeth. It’s not just one single wire; it’s a sophisticated system, a testament to the body’s incredible design. Understanding these neural pathways gives us a greater appreciation for what’s happening beneath the surface of our smiles.
The Master Conductor: The Trigeminal Nerve
The primary nerve responsible for almost all sensation in your face, including your teeth, is the trigeminal nerve. Also known as the fifth cranial nerve (CN V), it’s a major player in your sensory world. Think of it as a main highway for information traveling from your face to your brain. This nerve is a paired structure, meaning you have one on each side of your head, and it splits into three main branches, each covering a different territory.
These three branches are:
- The Ophthalmic Nerve (V1): This branch primarily handles sensation for the upper part of your face – your scalp, forehead, upper eyelids, and the front of your nose. It doesn’t directly innervate the teeth, so we’ll focus on its siblings.
- The Maxillary Nerve (V2): This is our first key player for dental sensation. It’s responsible for the middle part of your face, including your upper teeth, upper jaw (maxilla), palate, sinuses, and parts of your nasal cavity.
- The Mandibular Nerve (V3): The largest of the three branches, the mandibular nerve, takes care of the lower part of your face. Crucially, it provides sensation to your lower teeth, lower jaw (mandible), tongue (for general sensation, not taste), chin, and lower lip. It also has a motor component, controlling the muscles of mastication (chewing).
It’s this division of labor, particularly between the maxillary and mandibular nerves, that allows for such precise localization of sensations within the mouth.
Nerves of the Upper Jaw: Following the Maxillary Nerve (V2)
Once the maxillary nerve branches off from the trigeminal nerve, it embarks on a journey to supply sensation to the upper teeth. It doesn’t do this as one single entity but rather gives off several important smaller nerves that form a complex network.
Posterior Superior Alveolar (PSA) Nerve
The Posterior Superior Alveolar (PSA) nerve typically branches off the maxillary nerve in an area behind the upper jaw called the pterygopalatine fossa. It then travels downwards and forwards to enter small openings (foramina) on the back surface of the maxilla. From there, it dives into the bone to supply the pulps (the inner living tissue) of the upper molars – usually the third, second, and most of the first molar (except, sometimes, one particular root). It also provides sensation to the supporting gums and bone on the cheek-side of these teeth.
Middle Superior Alveolar (MSA) Nerve
The Middle Superior Alveolar (MSA) nerve is a bit of a variable character; it’s not present in everyone (studies suggest it’s missing in anywhere from 30% to over 50% of individuals). When present, it branches off the maxillary nerve (often from the infraorbital nerve, a main continuation of V2) within the infraorbital canal or groove. It then descends along the lateral wall of the maxillary sinus to supply the upper premolars (bicuspids) and, importantly, the mesiobuccal root of the first molar (the root that the PSA sometimes misses). It also innervates the surrounding buccal gingiva and bone.
The intricate branching of the trigeminal nerve, particularly its maxillary and mandibular divisions, is fundamental to dental sensation. These nerves don’t just serve teeth; they also provide sensory information from surrounding gums, bone, and facial skin. Understanding this complex anatomy is crucial for dental professionals when administering local anesthesia, aiming to numb specific areas effectively for patient comfort during procedures.
Anterior Superior Alveolar (ASA) Nerve
The Anterior Superior Alveolar (ASA) nerve also branches from the infraorbital nerve, but further forward, while the infraorbital nerve is still within its canal in the floor of the orbit (eye socket). The ASA nerve courses downwards and forwards within the front wall of the maxillary sinus. It’s responsible for providing sensation to the upper incisors (central and lateral) and the canine teeth. It also contributes to the sensation of the nearby gums, the lining of the maxillary sinus in that anterior region, and part of the nasal cavity.
These superior alveolar nerves (PSA, MSA, and ASA) don’t just run in isolation. They often form a delicate network, or dental plexus, above the roots of the upper teeth. From this plexus, tiny terminal branches then enter each individual tooth root to reach the pulp.
Nerves of the Lower Jaw: Navigating the Mandibular Nerve (V3)
The mandibular nerve (V3) has a more direct, though still complex, route to the lower teeth. Its primary dental branch is a significant nerve with its own distinct pathway.
Inferior Alveolar Nerve (IAN)
The star of the lower jaw’s sensory show is the Inferior Alveolar Nerve (IAN). It branches from the mandibular nerve and travels downwards, entering the mandible through an opening on its inner surface called the mandibular foramen. Once inside, it courses through the mandibular canal, a tunnel running horizontally within the bone, beneath the roots of the lower teeth. As it passes each tooth, the IAN sends off small dental branches that ascend into the roots, providing sensation to all the lower molars and premolars on one side. It also gives off branches to the surrounding bone.
Incisive Nerve
As the IAN travels forward, it eventually reaches an area near the premolars where it divides into two terminal branches. One of these is the incisive nerve. This nerve continues forward within the bone, often in its own bony canal, to supply the lower canine and incisor teeth on that side. It essentially takes over where the main IAN leaves off for the anterior teeth.
Mental Nerve
The other terminal branch of the IAN is the mental nerve. This nerve exits the mandible through an opening called the mental foramen, usually located below the lower premolars. Once it exits the bone, the mental nerve does not supply sensation to the teeth themselves. Instead, it provides sensation to the skin of the chin, the skin and mucous membrane of the lower lip, and the gingiva (gums) on the cheek-side of the lower anterior teeth and premolars. While not directly innervating tooth pulp, its proximity and origin make it relevant in dental contexts.
Other Related Nerves
While the IAN and its incisive branch are the direct suppliers to the lower tooth pulps, other branches of the mandibular nerve provide sensation to surrounding tissues:
- Lingual Nerve: This nerve runs close to the IAN initially but then veers towards the tongue. It provides general sensation (touch, pain, temperature – not taste for the anterior two-thirds, that’s the chorda tympani) to the anterior two-thirds of the tongue, the floor of the mouth, and the lingual gingiva (gums on the tongue side) of all lower teeth.
- Long Buccal Nerve (or Buccal Nerve): This nerve branches off the mandibular nerve and passes to the cheek. It provides sensation to the skin of the cheek, the mucous membrane lining the cheek, and importantly for dentistry, the buccal gingiva (gums on the cheek side) of the lower molars. It does not typically provide sensation to the teeth themselves.
Deep Inside: Nerves Within the Tooth Pulp
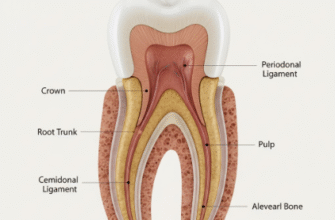
Regardless of whether it’s an upper or lower tooth, the nerve fibers ultimately have to get inside the tooth itself. They do this by entering through tiny openings at the very tip of each root, known as the apical foramen (plural: foramina). Several small nerve fibers, along with blood vessels, pass through these openings into the central chamber of the tooth, the pulp cavity.
The pulp is the living core of the tooth, containing connective tissue, blood vessels, and, of course, nerves. Once inside the pulp chamber, the nerve fibers branch extensively, especially in the coronal pulp (the part within the crown of the tooth). Just beneath the dentin layer (the hard tissue under the enamel), these nerve fibers form a rich network called the Plexus of Raschkow.
From this plexus, fine, unmyelinated nerve endings extend towards and sometimes into the innermost layer of dentin, often accompanying the processes of odontoblasts (the cells that form dentin) into the dentinal tubules. These tubules are microscopic channels that radiate from the pulp towards the enamel-dentin junction.
The primary sensation transmitted by these pulpal nerves is pain. This pain can range from a dull ache to a sharp, intense throb, depending on the nature and severity of the stimulus (like decay, trauma, or thermal changes). While the pulp can also sense extreme temperature changes, the predominant response to most stimuli is pain, acting as a crucial warning system for the tooth’s health.
Tooth sensitivity can arise from various factors, often when the protective enamel wears down or gums recede, exposing the dentin. The dentinal tubules then act as pathways for stimuli to reach the nerve endings in the pulp. This highlights the importance of good oral hygiene and regular dental check-ups to protect these intricate sensory structures and maintain oral health.
The exact mechanism of how stimuli like cold or touch on the dentin surface are translated into nerve signals is still debated, with the “hydrodynamic theory” being widely accepted. This theory suggests that stimuli cause fluid movement within the dentinal tubules, which in turn stimulates the nerve endings in or near the pulp.
Why This Neural Map Matters
Understanding this complex dental neuroanatomy isn’t just academic. It has profound practical implications:
- Pain Management: When a dentist needs to perform a procedure, they use local anesthetics to block nerve conduction in these specific pathways. Knowing which nerves supply which teeth allows for targeted injections, ensuring the area is numb and the patient is comfortable. For example, an IAN block numbs almost an entire lower quadrant, while infiltrations near specific upper teeth target the terminal branches of the superior alveolar nerves.
- Diagnosis: The nature and location of tooth pain can provide clues to its origin. However, because of nerve branching and overlap, pain can sometimes be “referred,” meaning it’s felt in a location different from the actual source. A thorough understanding of nerve pathways helps dentists differentiate and diagnose.
- Surgical Considerations: Dental surgeons must be acutely aware of the locations of major nerve trunks, like the IAN or mental nerve, to avoid damaging them during procedures such as wisdom tooth extractions or implant placements.
The sensory innervation of our teeth is a beautifully complex system. From the major trigeminal nerve down to the finest nerve endings within the tooth pulp, each component plays a vital role in our ability to sense our oral environment, protect our teeth from harm, and unfortunately, signal when things go wrong. Next time you feel that familiar twinge, take a moment to appreciate the sophisticated neural wiring at work.