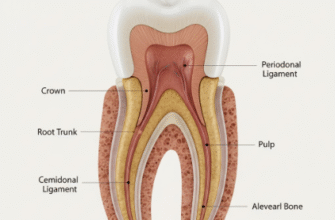
The ability to reliably bond restorative materials to tooth structure represents one of the most significant advancements in modern dentistry. Before the advent of sophisticated dental adhesives, dentists relied heavily on mechanical retention, meticulously carving undercuts and specific cavity shapes to ensure fillings wouldn’t dislodge. This often meant removing more healthy tooth structure than was strictly necessary to treat the decay. The journey from these purely mechanical approaches to today’s advanced adhesive systems is a fascinating story of chemical innovation and a deepening understanding of tooth biology.
The Quest for Stickiness: Early Attempts and Frustrations
In the early to mid-20th century, the concept of truly “gluing” a filling to a tooth was more of a dream than a reality. Materials like silicate cements and early acrylic resins offered some rudimentary adhesion, but it was weak, unpredictable, and often failed due to moisture contamination or the inherent challenges of bonding to a living, dynamic tissue like dentin. Dentists knew that if a reliable adhesive could be developed, it would revolutionize restorative procedures, allowing for more conservative preparations, better aesthetics, and improved marginal seal to prevent leakage and secondary decay. The challenge was immense: how to create a bond strong enough to withstand the harsh oral environment, including temperature fluctuations, chewing forces, and constant moisture?
A Revolutionary Spark: The Acid-Etch Technique
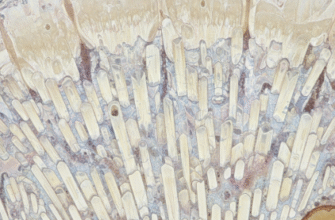
The breakthrough came in 1955. Dr. Michael Buonocore, working at the Eastman Dental Center, published a paper that would forever change the landscape of restorative dentistry. He demonstrated that treating enamel with an acid, specifically phosphoric acid, dramatically increased its surface energy and created microscopic porosities. This “etched” enamel surface provided a vastly improved substrate for mechanical interlocking with resin-based materials. Suddenly, the idea of micromechanical retention became a tangible reality, at least for enamel. This was the foundational discovery upon which all subsequent dental adhesive systems would be built.
Dr. Michael Buonocore’s 1955 publication on acid etching enamel is widely considered the cornerstone of modern adhesive dentistry. This groundbreaking discovery demonstrated that treating enamel with phosphoric acid significantly increased its surface energy and porosity. This allowed resin materials to micromechanically interlock with the tooth structure, paving the way for truly bonded restorations. It marked a pivotal shift from macro-mechanical retention to micro-mechanical adhesion.
Navigating the Generations: An Evolutionary Tale
Following Buonocore’s work, the development of dental adhesives can be broadly categorized into “generations,” each representing an attempt to improve bond strength, simplify clinical procedures, and expand bonding capabilities, especially to the more challenging dentin substrate.
First Generation: The Dawn of Enamel Bonding
The first generation of dental adhesives emerged in the late 1960s and early 1970s. These systems typically involved an enamel etchant and an unfilled or lightly filled resin that was thought to bond to enamel via an NPG-GMA (N-phenylglycine-glycidyl methacrylate) chelation mechanism to calcium. However, bond strengths were relatively low, particularly to dentin, and their clinical success was limited. They were primarily effective for enamel bonding, but the dream of reliable dentin adhesion remained elusive.
Second Generation: Grappling with Dentin
The second generation, appearing in the late 1970s and early 1980s, attempted to tackle the dentin bonding problem. These adhesives often used phosphate-based monomers, like halophosphorus esters of Bis-GMA or HEMA, with the aim of creating a chemical bond to the calcium in dentin. Unfortunately, these bonds were weak and highly susceptible to hydrolytic degradation (breakdown by water). The smear layer, a layer of debris created during tooth preparation, also proved to be a significant obstacle, and these systems didn’t manage it effectively. Clinical performance was generally poor, leading to frustration and a search for better solutions.
Third Generation: Primer Steps and Smear Layer Management
Introduced in the mid-to-late 1980s, third-generation adhesives represented a step forward. They typically involved an enamel etchant, a dentin primer, and an adhesive resin. The primer was designed to modify or partially remove the smear layer and improve the wetting of the dentin surface by the adhesive resin. While bond strengths improved compared to previous generations, these systems were complex, involving multiple bottles and steps. The longevity of the dentin bond was still a concern, and technique sensitivity was high.
Fourth Generation: The “Total-Etch” or “Etch-and-Rinse” Gold Standard
The early 1990s saw the arrival of fourth-generation adhesives, which became a benchmark for many years. These systems employed a “total-etch” or “etch-and-Rinse” approach. This involved:
- Etching: Phosphoric acid was used to etch both enamel and dentin simultaneously. This removed the smear layer completely and demineralized the superficial dentin.
- Priming: A hydrophilic (water-loving) primer, typically containing monomers like HEMA dissolved in a solvent (acetone, ethanol, or water), was applied to the etched and rinsed dentin. The primer chased water from the dentin surface and infiltrated the exposed collagen network.
- Bonding: An unfilled or lightly filled hydrophobic (water-repelling) adhesive resin was then applied to penetrate the primed surface and co-polymerize with the overlying composite resin.
Fifth Generation: Simplifying with “One-Bottle” Etch-and-Rinse
Seeking to simplify the multi-step fourth-generation systems, fifth-generation adhesives emerged in the mid-to-late 1990s. These are also known as “one-bottle” etch-and-rinse systems because they combined the primer and adhesive resin into a single bottle. The etching step with phosphoric acid for both enamel and dentin remained separate. This reduced the number of components and application steps, making the process more user-friendly. While generally offering good performance, some concerns arose regarding the long-term stability of these combined primer/adhesives due to their inherent hydrophilicity and potential for water sorption and phase separation within the bottle.
Sixth Generation: The Rise of Self-Etch
A significant paradigm shift occurred with sixth-generation adhesives, introduced in the late 1990s and early 2000s. These were the first commercially successful self-etch adhesives. The key innovation was the incorporation of acidic monomers that could simultaneously demineralize and infiltrate tooth structure, eliminating the need for a separate phosphoric acid etching and rinsing step, particularly for dentin. This was seen as a way to reduce technique sensitivity associated with the rinse-and-dry step of total-etch systems and potentially decrease post-operative sensitivity. Sixth-generation systems came in two main types:
- Type I (Self-Etching Primer + Adhesive): These involved applying a self-etching primer, followed by a separate adhesive resin. The primer conditioned and primed the tooth, and the adhesive bonded to it.
- Type II (Two-Component, One-Step Self-Etch): These typically involved mixing two liquids immediately before application or having two components applied sequentially without rinsing in between. They effectively combined etching, priming, and bonding into a single application step after mixing.
Seventh Generation: All-in-One Simplicity
The quest for ultimate simplification led to seventh-generation adhesives, often termed “all-in-one” or “one-step self-etch” adhesives. These systems combined etchant, primer, and adhesive into a single bottle and required no mixing. The clinician simply applied the liquid to the tooth, air-thinned it, and light-cured. While offering maximum convenience, these highly acidic and hydrophilic formulations raised concerns about their long-term bond durability, water degradation, and ability to effectively etch enamel. Bond strengths, particularly to enamel, were sometimes lower than with multi-step systems. They also tended to be more permeable, acting like semi-permeable membranes, which could lead to water movement across the interface over time.
The Modern Era: Universal Adhesives (Eighth Generation and Beyond)
The current pinnacle in adhesive technology is represented by universal adhesives, sometimes referred to as multi-mode or eighth-generation adhesives. These products are designed for versatility and aim to provide reliable bonding to a wide array of substrates, including enamel, dentin, composite resin, metals, and ceramics (like zirconia and glass-ceramics). A key feature is their flexibility in application mode:
- Total-etch (etch-and-rinse): Can be used with a prior phosphoric acid etching step on enamel and dentin.
- Self-etch: Can be applied directly without a separate etching step.
- Selective-etch: Phosphoric acid is applied only to enamel margins, while the adhesive acts in self-etch mode on dentin.
Persistent Challenges and the Horizon
Despite enormous progress, challenges in dental adhesion persist. Ensuring the long-term durability of the bond, especially to dentin, in the hydrolytically challenging oral environment remains a primary goal. Minimizing technique sensitivity and post-operative sensitivity are ongoing pursuits. The future may see the wider adoption of bioactive adhesives – materials that not only bond but also possess therapeutic properties, such as ion release (e.g., fluoride, calcium, phosphate) to promote remineralization, or antibacterial components to inhibit secondary caries. Further simplification without compromising efficacy will undoubtedly continue to drive innovation.
A Sticky Success Story
The evolution of dental adhesives is a testament to persistent research and development. From the foundational discovery of acid etching to the sophisticated universal adhesives of today, each generation has built upon the successes and addressed the limitations of its predecessors. These advancements have profoundly impacted restorative dentistry, enabling more conservative tooth preparations, expanding the range of treatable conditions, and improving the longevity and aesthetics of dental restorations. The journey to create the perfect “glue” for teeth continues, promising even more exciting developments in the years to come.