Nestled within our jaws, a specialized type of bone diligently works to keep our teeth firmly in place. This unsung hero is the alveolar bone, and while it might not be the most famous part of our skeletal system, its role is absolutely crucial for a functional smile and effective chewing. Understanding its basic anatomy reveals a surprisingly complex and dynamic structure, perfectly engineered for the demands placed upon it daily. It’s not just a static holder; it’s a living tissue that responds and adapts throughout our lives.
The Alveolar Process: Foundation of Support
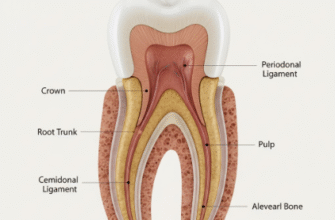
The story of alveolar bone begins with the larger bones of the skull: the maxilla (upper jaw) and the mandible (lower jaw). The alveolar bone is not a separate bone itself, but rather the specialized part of these jawbones that forms to house the roots of the teeth. This entire tooth-bearing extension is known as the alveolar process. Think of it as the dedicated neighborhood within the city of your jaw, specifically built for teeth to reside in.
The development of the alveolar process is intricately tied to the development and eruption of teeth. If a tooth fails to develop, the corresponding section of the alveolar process often doesn’t form either, or it remains underdeveloped. Similarly, when a tooth is lost, the alveolar process in that area tends to gradually resorb, or shrink, over time because its primary purpose is no longer being fulfilled. This highlights its unique dependency on the presence of teeth.
The alveolar process can be broadly divided into two main parts based on its relationship to the teeth:
- Basal bone: This is the main body of the maxilla or mandible, located beneath or apical to the roots of the teeth. It provides the foundational support for the alveolar process itself.
- Alveolar bone proper: This is the thin layer of compact bone that directly lines the tooth socket, also known as the alveolus.
The overall shape and thickness of the alveolar process vary considerably depending on the location in the mouth, the size and shape of the teeth it supports, and the forces it endures. For instance, the bone around molars, which bear significant chewing forces, is generally thicker and more robust than the bone around incisors.
Key Layers and Components of Alveolar Bone
Zooming in on the alveolar process, we find a sophisticated structure composed of different types of bone tissue, each with specific characteristics and functions. These components work in concert to provide a secure yet adaptable anchoring system for the teeth.
Alveolar Bone Proper: The Tooth’s Immediate Cradle
The alveolar bone proper is the star player when it comes to direct tooth support. It’s a thin, compact layer of bone that forms the inner wall of the tooth socket, also called the alveolus. On a dental radiograph (X-ray), this layer appears as a dense white line surrounding the tooth root and is often referred to as the lamina dura. The term “lamina dura” literally means “hard layer,” reflecting its dense nature.
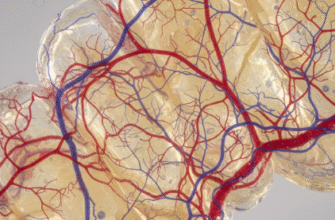
A fascinating feature of the alveolar bone proper is its perforated structure. It’s riddled with numerous small openings, giving it a sieve-like appearance, which is why it’s also known as the cribriform plate. These openings allow blood vessels and nerves to pass from the cancellous bone into the periodontal ligament, the fibrous tissue that surrounds the tooth root and connects it to the alveolar bone proper. This rich vascular supply is vital for the health and maintenance of both the bone and the periodontal ligament.
Crucially, the alveolar bone proper is where the principal fibers of the periodontal ligament, known as Sharpey’s fibers, embed themselves. These collagenous fibers act like tiny suspensory ligaments, anchoring the tooth firmly within its socket while allowing for slight physiological movement during functions like chewing. The ends of these fibers that insert into the bone become mineralized, creating a very strong attachment.
Cortical Plates: The Protective Outer Shell
Encasing the alveolar process on its outer (facial or buccal) and inner (lingual or palatal) sides are the cortical plates. These are layers of dense, compact bone that provide strength and protection to the more delicate structures within. The thickness of the cortical plates varies significantly throughout the mouth. Generally, they are thicker in the mandible than in the maxilla, and thicker in the posterior regions compared to the anterior regions.
The cortical bone is covered by a thin connective tissue membrane called the periosteum. The periosteum has an outer fibrous layer and an inner cellular layer containing osteoblasts (bone-forming cells), which are crucial for bone growth and repair. This membrane also carries blood vessels and nerves that supply the cortical bone.
Cancellous Bone: The Inner Spongy Network
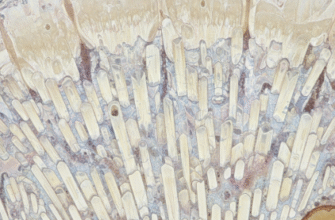
Nestled between the alveolar bone proper and the cortical plates lies the cancellous bone, also known as spongy bone or trabecular bone. This type of bone is much less dense than compact bone, characterized by a porous, honeycomb-like structure. It consists of a network of bony spicules or plates called trabeculae, which enclose irregular marrow spaces.
The arrangement and density of these trabeculae are not random; they are oriented to best resist and distribute the forces transmitted from the teeth during function. The marrow spaces within the cancellous bone are typically filled with red hematopoietic marrow in younger individuals, which produces blood cells, and gradually transitions to yellow fatty marrow with age. Despite this change, the marrow spaces remain rich in blood vessels, contributing significantly to the overall vascular supply of the alveolar bone.
The cancellous bone acts as a shock absorber, helping to dissipate the forces of mastication and protecting the more rigid cortical plates and the tooth roots. Its porous nature also makes it more metabolically active than compact bone, allowing for quicker remodeling in response to changes in functional demands or during orthodontic tooth movement.
The alveolar bone is a truly unique osseous tissue because its existence and architecture are fundamentally dependent on the presence of teeth. It forms as teeth erupt and begins to resorb if teeth are lost. This dynamic interplay underscores the specific role this bone plays in oral function.
Cellular Architects of Bone
Like all bone tissue, alveolar bone is a living, dynamic material constantly undergoing processes of formation and resorption. This activity is orchestrated by specialized bone cells:
Osteoblasts: The Builders
Osteoblasts are the bone-forming cells. They originate from precursor cells found in the periosteum and the bone marrow. Their primary function is to synthesize and secrete the organic matrix of bone, known as osteoid. Osteoid is primarily composed of collagen fibers, along with other proteins. Once osteoid is laid down, osteoblasts then play a crucial role in its mineralization, a process where calcium phosphate crystals (hydroxyapatite) are deposited within the matrix, giving bone its characteristic hardness and rigidity.
Active osteoblasts are typically found on the surfaces of growing or remodeling bone. When their bone-forming activity is complete, some osteoblasts become entrapped within the matrix they have created and transform into osteocytes. Others may remain on the bone surface as lining cells or undergo apoptosis (programmed cell death).
Osteocytes: The Maintainers
Osteocytes are mature bone cells derived from osteoblasts that have become embedded within the mineralized bone matrix. Each osteocyte resides in a small space called a lacuna. These cells extend long, slender cytoplasmic processes through tiny channels in the bone called canaliculi. These canaliculi connect adjacent lacunae, forming a network that allows osteocytes to communicate with each other and with cells on the bone surface.
Osteocytes are considered the primary mechanosensors in bone. They can detect mechanical stresses and strains placed on the bone and signal other cells, like osteoblasts and osteoclasts, to initiate remodeling processes. They also play a vital role in maintaining the vitality of the bone matrix by regulating mineral exchange.
Osteoclasts: The Remodelers
Osteoclasts are large, multinucleated cells responsible for bone resorption, the process of breaking down bone tissue. They are derived from hematopoietic stem cells, the same lineage that produces macrophages. Osteoclasts attach to the bone surface and create a sealed-off acidic environment beneath them. They release enzymes, such as acid phosphatase, and acids that dissolve the mineral component and digest the organic matrix of the bone.
The area where an osteoclast is actively resorbing bone is often a shallow depression known as a Howship’s lacuna. Bone resorption by osteoclasts is a critical part of normal bone turnover, growth, repair, and remodeling. It allows for the removal of old or damaged bone and the reshaping of bone in response to functional demands or orthodontic forces.
Blood Supply and Innervation
The alveolar bone boasts a rich blood supply, essential for its metabolic activity and healing capacity. Arterial blood reaches the alveolar process through branches of the maxillary and mandibular arteries. These larger vessels give off smaller branches that penetrate the cortical plates through Volkmann’s canals and Haversian canals to supply the compact bone. The cancellous bone and alveolar bone proper receive an abundant supply from vessels within the marrow spaces and from branches that pass through the cribriform plate from the periodontal ligament.
Nerve supply to the alveolar bone largely follows the pathways of the blood vessels. Sensory nerves, primarily branches of the trigeminal nerve, provide innervation. These nerves are responsible for sensations such as pain and pressure, although the bone tissue itself is relatively insensitive compared to the highly sensitive periodontal ligament.
A Dynamic and Responsive Tissue
One of the most remarkable characteristics of alveolar bone is its plasticity – its ability to change its structure in response to various stimuli. This is evident in several ways. During tooth eruption, bone is resorbed to create a path for the emerging tooth and then formed around the root as it establishes its position. If a tooth is subjected to orthodontic forces, the alveolar bone on the side of pressure undergoes resorption, while new bone is deposited on the side of tension, allowing the tooth to move through the jaw.
Even normal chewing forces induce microscopic changes and remodeling within the alveolar bone, helping to maintain its density and functional adaptation. This constant turnover ensures that the bone remains healthy and capable of supporting the teeth effectively. The intricate balance between bone formation by osteoblasts and bone resorption by osteoclasts is key to this adaptability. Understanding this dynamic nature is fundamental in many aspects of dental practice, emphasizing how this specialized bone works tirelessly to support our dentition throughout life.