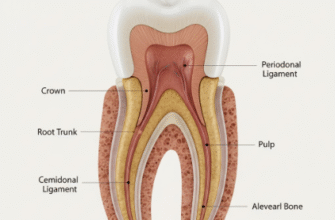
The neck of the tooth, more formally known as the cervical line or Cementoenamel Junction (CEJ), is a subtle yet profoundly important anatomical landmark. Think of it as the waistline of your tooth, the distinct boundary where the glistening, hard enamel covering the crown gracefully meets the cementum, the less glamorous but equally vital tissue covering the root. This junction isn’t just a simple meeting point; it’s a critical zone influencing tooth health, stability, and even how your smile looks. Understanding its structure and vulnerabilities can empower individuals to take better care of this often-overlooked region.
Defining the Neck: More Than Just a Line
While we casually refer to the “neck” of the tooth, its precise anatomical definition lies in the CEJ. The enamel, the hardest substance in the human body, forms the outer layer of the tooth’s crown – the part visible above the gum line in a healthy mouth. Below this, the cementum, a bone-like tissue, covers the tooth’s root, anchoring it within the jawbone via the periodontal ligament. The cervical line is precisely where these two distinct tissues abut or overlap.
It’s also important to distinguish between the anatomical crown (the part covered by enamel) and the clinical crown (the part of the tooth visible in the mouth, not covered by gingiva). In a young, healthy mouth, the cervical line is typically just apical to (below) the edge of the gum, meaning a small portion of the anatomical crown might be covered by gingiva. As people age or if gum recession occurs, the cervical line and even parts of the root can become exposed, altering the landscape of the clinical crown.
The Microscopic Encounter: How Enamel Meets Cementum
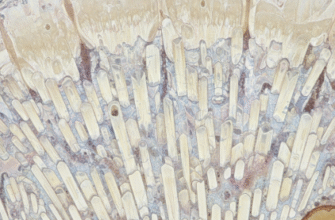
The meeting of enamel and cementum at the CEJ isn’t always a perfectly neat affair. Microscopically, there are three main ways these tissues can relate to each other, and the prevalence of each varies:
- Cementum overlaps enamel: This is the most common scenario, found in about 60-65% of cases. A thin layer of cementum extends slightly over the enamel. This configuration is thought to offer a good seal.
- Edge-to-edge butt joint: In approximately 30% of instances, the enamel and cementum meet in a direct, flush end-to-end manner.
- Gap between enamel and cementum: This occurs in about 5-10% of teeth. Here, there’s a small space where neither enamel nor cementum covers the underlying dentin. This exposed dentin can be a prime site for tooth sensitivity.
The formation of these tissues during tooth development – ameloblasts producing enamel and cementoblasts producing cementum – dictates the nature of this junction. The point at which their activity ceases or transitions defines the cervical line.
Clinical Crossroads: Why the Cervical Line Matters So Much
The cervical region of the tooth is a hotbed of clinical activity and concern for several reasons. Its unique anatomy and location make it particularly susceptible to a range of dental issues.
The Gum’s Embrace and Plaque’s Playground
In an ideal state, the gingiva (gum tissue) forms a tight cuff around the tooth, with its margin resting at or slightly covering the cervical line. This creates a natural seal. However, the slight contour change at the CEJ can also be an area where dental plaque – a sticky film of bacteria – readily accumulates, especially if oral hygiene isn’t meticulous. This plaque biofilm is the primary culprit behind gum inflammation (gingivitis) and, if left unchecked, can progress to periodontitis, a more severe gum disease that affects the supporting bone.
The Perils of Recession
Gingival recession, the pulling back of the gums from the tooth surface, is a common problem that directly exposes the cervical line and, often, the root surface. When the root is exposed, several problems can arise. The cementum covering the root is much softer and thinner than enamel, making it more vulnerable to wear and decay. Furthermore, recession often uncovers the dentin, which contains microscopic tubules leading to the tooth’s nerve, resulting in sensitivity to hot, cold, or sweet stimuli.
Vulnerability to Lesions: Cavities and Beyond
The cervical area is prone to specific types of lesions:
- Cervical Caries (Root Cavities): When the root surface becomes exposed due to recession, it is more susceptible to decay than enamel. These cavities form on the cementum or dentin at or below the cervical line. They can progress rapidly due to the softer nature of these tissues.
- Non-Carious Cervical Lesions (NCCLs): These are a fascinating and often multifactorial group of lesions that cause a loss of tooth structure at the cervical line, but are not caused by bacteria.
- Abrasion: This is mechanical wear, often caused by overly aggressive toothbrushing with a hard-bristled brush, or using highly abrasive toothpaste. It typically presents as a V-shaped or wedge-shaped notch.
- Erosion: This is chemical wear, caused by acids (not from bacteria). These can be extrinsic acids (from acidic foods, drinks like sodas or fruit juices, or even some medications) or intrinsic acids (from stomach acid due to conditions like acid reflux or bulimia). Eroded lesions are often saucer-shaped and smooth.
- Abfraction: This is a more controversial type of lesion, thought to be caused by excessive occlusal (biting) forces that cause the tooth to flex. This flexing is theorized to concentrate stress at the cervical fulcrum point, leading to microfractures and the chipping away of tooth structure. Abfraction lesions are often deep and wedge-shaped.
Often, NCCLs are a result of a combination of these factors. For instance, acid erosion might soften the tooth surface, making it more susceptible to abrasion from brushing.
The cervical line, or neck of the tooth, is a particularly vulnerable area. Exposure due to gum recession can lead to heightened sensitivity and an increased risk for root cavities. Aggressive brushing or acidic challenges can further wear down this delicate junction, emphasizing the need for gentle care and awareness.
The Sensitivity Factor
As mentioned, exposed dentin is a primary cause of tooth sensitivity. The cervical region is a common site for this because of the potential for CEJ gaps, gum recession exposing root surfaces, and the development of NCCLs which wear away protective enamel or cementum. The tiny tubules in the dentin transmit temperature changes or osmotic pressure changes directly to the tooth’s pulp (nerve), triggering that familiar sharp, short pain.
Restorative Challenges and Aesthetics
When restorations like fillings or crowns are needed, the cervical margin (the edge of the restoration closest to the root) is a critical area. Achieving a perfect seal here is paramount to prevent leakage, recurrent decay, and irritation to the gums. Placing restorations that extend to or below the gum line requires meticulous technique. Aesthetically, the appearance of the cervical area is also important, especially for front teeth. Discoloration, exposed root surfaces, or visible margins of restorations can detract from a natural, healthy-looking smile. The contour and color transition from crown to root at the cervical line must be managed carefully for optimal cosmetic results.
Variations Across the Dentition
The curvature and prominence of the cervical line are not uniform across all teeth or even on all surfaces of a single tooth. For example:
- On anterior teeth (incisors and canines), the cervical line typically has a more pronounced curvature on the mesial (towards the midline) and distal (away from the midline) surfaces, allowing for the height of the interdental papilla (the gum tissue between teeth). The curvature is less pronounced on the facial (lip-side) and lingual (tongue-side) surfaces.
- On posterior teeth (premolars and molars), the cervical line generally has a less dramatic curvature on all surfaces, appearing somewhat straighter, especially on the buccal (cheek-side) and lingual surfaces.
These variations accommodate the different shapes and functions of the teeth and the surrounding gingival architecture.
Nurturing the Neck: Protecting the Cervical Line
Given its vulnerabilities, protecting the cervical region is a key aspect of maintaining long-term oral health. Several practices are crucial:
- Gentle and Effective Brushing: Using a soft-bristled toothbrush and a gentle, circular or modified Bass technique can effectively remove plaque without abrading tooth structure or damaging the gums. Avoid aggressive horizontal scrubbing.
- Thorough Interdental Cleaning: Flossing or using interdental brushes is essential to clean the plaque that accumulates between teeth, right up to and slightly below the cervical line where the gum meets the tooth.
- Managing Acid Exposure: Limiting intake of acidic foods and drinks, rinsing with water after consuming them, and addressing conditions like acid reflux can help prevent erosion.
- Regular Dental Check-ups: Professional cleanings remove hardened plaque (tartar) that cannot be removed by brushing alone. Dentists can also identify early signs of recession, NCCLs, or cervical caries, allowing for timely intervention.
- Addressing Bruxism or Clenching: If abfraction is suspected due to grinding or clenching, a dentist might recommend a nightguard or other therapies to manage occlusal forces.
The cervical line of the tooth, though a small anatomical feature, plays an outsized role in dental health and disease. Its integrity is fundamental for preventing sensitivity, decay, and gum problems. By understanding its structure and the factors that can compromise it, we can take more informed steps to preserve the health and longevity of our smiles, right down to the neck of each tooth.