Long before a tiny white speck heralds the arrival of a new tooth, a hidden world of intricate biological engineering is in full swing deep within the developing jaws. This subterranean phase of tooth development, or odontogenesis, is a marvel of cellular communication, differentiation, and construction. It’s a complex ballet where tissues interact, cells transform, and the very foundations of our future smile are meticulously laid down, all without a single glimpse from the outside world. Understanding this pre-eruptive journey reveals the true artistry behind every single tooth.
The First Stirrings: From Lamina to Bud
The story of a tooth begins with a subtle thickening in the epithelial lining of the embryonic oral cavity. This band of cells, known as the dental lamina, is the very first architectural hint of where teeth will eventually form. Think of it as the initial chalk mark on a construction site. At specific points along this lamina, groups of epithelial cells begin to proliferate and push downwards into the underlying mesenchymal tissue, which is a type of embryonic connective tissue. This downward projection of epithelial cells, surrounded by condensing mesenchyme, marks the bud stage.
At this point, the developing tooth doesn’t resemble a tooth at all; it’s more like a small, roundish swelling or bud. However, this unassuming structure holds immense potential. The epithelial component will eventually give rise to the enamel, while the mesmerized mesenchyme, now called the ectomesenchyme because of its neural crest origin, will form the dentin, pulp, and other supporting structures of the tooth. The interaction between these two tissue types is crucial; they engage in a constant dialogue, exchanging signals that guide every subsequent step of development.
Taking Shape: The Emergence of the Cap
As development progresses, the epithelial bud doesn’t just grow larger; it begins to change shape due to uneven cell proliferation. The deeper surface of the bud invaginates, or folds inward, transforming the simple bud into a more complex, three-dimensional structure resembling a cap. This is aptly named the cap stage. Now, three distinct components become clearly identifiable: the enamel organ, the dental papilla, and the dental follicle (also known as the dental sac).
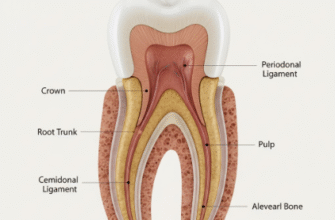
The enamel organ, derived from the epithelium, sits like a cap over the condensing ectomesenchymal cells of the dental papilla. The dental papilla itself is that condensed area of ectomesenchyme partially enclosed by the invaginated part of the enamel organ. It’s destined to form the tooth’s dentin and pulp. Surrounding both the enamel organ and the dental papilla is a more fibrous layer of ectomesenchyme called the dental follicle. This sac-like structure will eventually give rise to the supporting tissues of the tooth: the cementum (which covers the root), the periodontal ligament (which anchors the tooth to the bone), and a portion of the alveolar bone that forms the tooth socket.
A Symphony of Cells: The Intricate Bell Stage
The cap stage evolves into the bell stage, so named because the enamel organ deepens its invagination and expands, taking on a bell-like appearance. This stage is characterized by significant histodifferentiation and morphodifferentiation. Histodifferentiation means that cells are transforming into specialized types, while morphodifferentiation refers to the establishment of the tooth’s specific size and shape, particularly that of its crown.
The enamel organ itself becomes a more complex, multi-layered structure. We can now distinguish four distinct layers:
- The Outer Enamel Epithelium (OEE): A layer of cuboidal cells on the periphery of the enamel organ, serving a protective role and involved in maintaining the organ’s shape.
- The Inner Enamel Epithelium (IEE): A layer of columnar cells lining the concavity of the bell. These are the crucial cells that will differentiate into ameloblasts, the specialized cells responsible for producing enamel.
- The Stellate Reticulum (SR): Star-shaped cells that fill the bulk of the enamel organ, between the OEE and IEE. These cells secrete glycosaminoglycans, which draw water into the area, creating a cushioned, shock-absorbing environment that protects the differentiating IEE cells. They also play a role in nutrient transport.
- The Stratum Intermedium (SI): A layer of squamous to cuboidal cells found directly adjacent to the IEE. This layer is essential for enamel formation, providing alkaline phosphatase and other support to the ameloblasts.
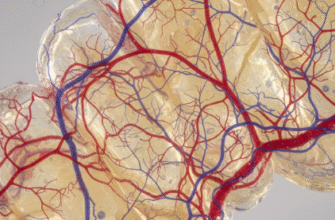
Simultaneously, within the dental papilla, significant changes are occurring. The peripheral cells of the dental papilla, directly adjacent to the IEE, differentiate into tall columnar cells called odontoblasts. These are the cells that will produce dentin. The central portion of the dental papilla will eventually become the tooth’s pulp, rich in blood vessels and nerves. The boundary where the IEE and the newly differentiated odontoblasts meet is critically important; it will become the Dentinoenamel Junction (DEJ), the interface between enamel and dentin in the mature tooth. It is during the late bell stage that the overall morphology of the crown – whether it will be an incisor, canine, premolar, or molar – is firmly established before any hard tissue formation begins.
The Bell Stage is a cornerstone of tooth development, where cellular destiny is largely decided. The intricate signaling between the inner enamel epithelium and the dental papilla cells triggers their transformation into enamel-forming ameloblasts and dentin-forming odontoblasts. This precise differentiation is fundamental, as any disruption can lead to abnormalities in tooth structure and shape. The blueprint for the tooth’s crown is finalized during this period.
Layer by Layer: Crafting Dentin and Enamel
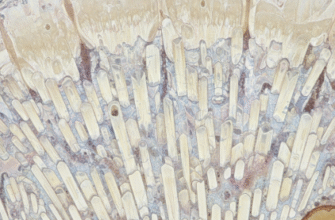
With the cellular machinery in place, the next phase involves the actual deposition of the hard tissues of the tooth. This is known as apposition, where enamel and dentin are laid down incrementally, layer by layer. An important principle here is that dentinogenesis (dentin formation) always precedes amelogenesis (enamel formation).
Dentin’s Debut
The newly differentiated odontoblasts in the dental papilla begin their work first. They retreat away from the future DEJ, towards the center of the papilla, leaving behind an organic matrix called predentin. This predentin is primarily composed of collagen fibers. Soon after its deposition, the predentin begins to mineralize, transforming into mature dentin. As odontoblasts move inward, they leave behind a cytoplasmic extension called an odontoblastic process, which becomes encased within a small channel in the dentin known as a dentinal tubule. This is why dentin, unlike enamel, is considered a living, sensitive tissue throughout life, as these processes extend far into its structure.
Enamel’s Arrival
The deposition of the very first layer of dentin by odontoblasts acts as a crucial signal. This signal prompts the adjacent IEE cells, which have now fully differentiated into ameloblasts, to begin their secretory activity. The ameloblasts start to lay down an enamel matrix, moving outwards, away from the dentin. Enamel matrix is chemically different from dentin matrix; it’s rich in unique proteins like amelogenins and enamelins, and has a different structural organization. As the ameloblasts deposit enamel, they also move away from the DEJ, creating the enamel layer that will cap the dentin.
Both dentin and enamel are laid down rhythmically, in daily increments, leading to visible lines (like the incremental lines of von Ebner in dentin and striae of Retzius in enamel) in the mature tooth, reflecting this layered construction. The interface where they meet, the DEJ, is often scalloped, which helps to create a strong, interlocking bond between these two dissimilar hard tissues, crucial for withstanding the forces of mastication. Following the deposition of the organic matrices, both tissues undergo extensive mineralization, where hydroxyapatite crystals are incorporated, giving enamel its extreme hardness and dentin its resilient toughness. Enamel becomes the hardest substance in the human body, while dentin provides the underlying support and flexibility.
The Foundation Below: Root Genesis
Once the crown of the tooth is largely formed, the focus of development shifts to creating the root, the part of the tooth that will anchor it within the jawbone. The structure responsible for orchestrating root development is Hertwig’s Epithelial Root Sheath (HERS). HERS is formed by the apical proliferation of the outer and inner enamel epithelium from the cervical loop region of the enamel organ – essentially where the OEE and IEE meet at the rim of the enamel organ.
HERS grows downwards, away from the crown, outlining the shape of the future root (or roots, in the case of multi-rooted teeth). As HERS extends, its inner layer of cells induces the adjacent dental papilla cells to differentiate into odontoblasts, which then begin to form root dentin. Unlike in the crown, the IEE cells of HERS do not differentiate into ameloblasts, so no enamel is formed on the root surface. Instead, as root dentin is laid down, HERS begins to fragment and break down. This fragmentation allows cells from the surrounding dental follicle to come into contact with the newly formed root dentin surface. These dental follicle cells then differentiate into cementoblasts, which deposit a layer of cementum onto the root dentin. Cementum is a bone-like tissue that provides an attachment surface for the fibers of the periodontal ligament.
The remnants of HERS that don’t completely disappear may persist as clusters of epithelial cells in the periodontal ligament, known as the Epithelial Rests of Malassez. These rests are usually dormant but can sometimes become cystic later in life. As the root lengthens, the opening at its apex, the apical foramen, gradually narrows, but remains as the portal through which blood vessels and nerves will enter the pulp chamber of the fully formed tooth.
Silent Shifts: Pre-Eruptive Positioning
Even as the tooth crown and root are forming deep within the crypts of the jawbone, the developing tooth is not entirely static. It undergoes subtle but significant pre-eruptive tooth movements. These are not the active, forceful movements of eruption that will eventually bring the tooth into the oral cavity, but rather slow, adjusting movements that occur while the tooth is still completely encased in bone. These movements help to position the developing tooth germ correctly as the jaws grow and as adjacent teeth also develop. The tooth might drift bodily, or tilt, ensuring it’s in the optimal spot for its eventual emergence and function. This phase ensures that the meticulously crafted tooth is perfectly aligned for its journey towards the surface, ready to take its place in the dental arch.
The journey of a tooth from a mere epithelial thickening to a fully formed structure, complete with its crown and root, all before it even peeks through the gums, is a testament to the precision of biological processes. Each stage, from bud to bell, and each cellular interaction, is critical in shaping an organ that is both incredibly strong and intricately designed. This hidden phase of development lays down the essential anatomy, preparing the tooth for its eventual debut and a lifetime of function.