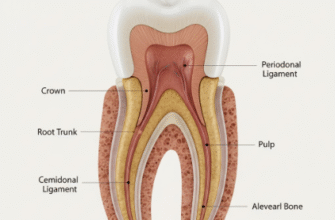
When we flash a smile or bite into a crisp apple, we rarely pause to consider the intricate architecture packed into each individual tooth. Far from being simple, inert pegs, our teeth are marvels of biological engineering, composed of several distinct layers, each with a specific role and characteristics. Understanding these layers is not just for dental students; it can help us appreciate the importance of good oral hygiene and why certain dental issues arise. Let’s peel back the curtain, metaphorically speaking, and explore the fascinating world within a single tooth.
The Mighty Shield: Enamel
The outermost layer of the crown of your tooth – the part visible above the gumline – is called enamel. Think of it as the tooth’s personal bodyguard. It is the hardest substance in the entire human body, even tougher than bone! This incredible hardness is thanks to its composition, which is about 96 percent minerals, primarily a crystalline calcium phosphate known as hydroxyapatite. The remaining percentage is water and organic material.
Enamel’s primary job is to protect the sensitive inner layers of the tooth from the daily onslaught of chewing forces, temperature extremes like hot coffee or ice cream, and the acids produced by bacteria in our mouths. Despite its strength, enamel is not invincible. It is somewhat brittle and can chip or crack under excessive force. More commonly, it faces the threat of demineralization – the dissolving of its mineral content – by acids. These acids can come directly from acidic foods and drinks, such as citrus fruits or soda, or be byproducts of oral bacteria feasting on sugars and starches left on your teeth.
Enamel is truly remarkable. While incredibly hard, it is acellular, meaning it contains no living cells. This characteristic means that once enamel is damaged or worn away, the body cannot regenerate it. This is why preventing cavities and enamel erosion is so crucial for long-term dental health.
The color of enamel can range from a light yellow to a grayish-white. Its translucency means that the color of the underlying dentin can also influence the overall perceived shade of the tooth. Because it lacks living cells, enamel cannot feel pain. So, if you experience tooth sensitivity, it usually means the problem has progressed beyond the enamel to the more sensitive layers beneath.
Beneath the Armor: Dentin
Peel away the enamel, and you will find dentin, a layer that makes up the bulk of the tooth structure. It is a hard, dense, bony tissue, but softer than enamel. Think of it as the tooth’s core strength, providing support to the enamel and protecting the innermost pulp. While enamel is mostly mineral, dentin has a more complex composition: roughly 70 percent inorganic materials, mainly hydroxyapatite and calcium phosphate, 20 percent organic materials, primarily collagen protein, and 10 percent water.
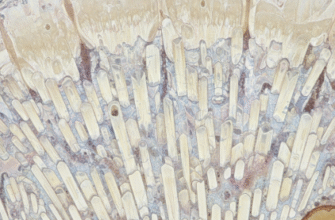
The Role of Dentinal Tubules
A fascinating feature of dentin is its microscopic structure. It is permeated by thousands of tiny, parallel channels called dentinal tubules. These tubules radiate outward from the pulp cavity, the tooth’s center, towards the external enamel or cementum. Each tubule contains fluid and a slender extension of an odontoblast cell, whose main body resides in the pulp. This tubular structure is key to understanding tooth sensitivity. When enamel wears thin or gums recede, exposing dentin, external stimuli like hot, cold, sweet, or acidic substances can cause movement of the fluid within these tubules. This movement can trigger the nerve endings in the pulp, leading to that sharp, often unpleasant, sensation of tooth sensitivity.
Dentin is typically pale yellow and is largely responsible for the overall color of your teeth, as the enamel covering it is somewhat translucent. Unlike enamel, dentin is a living tissue and can, to a limited extent, repair itself. When irritated by decay or trauma, the odontoblasts in the pulp can lay down more dentin, known as tertiary dentin or reparative dentin, to protect the pulp. There are different types: reactionary dentin, formed by pre-existing odontoblasts, and reparative dentin, formed by newly differentiated odontoblast-like cells when the original odontoblasts are damaged.
The Living Core: Dental Pulp
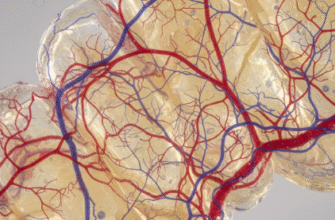
At the very heart of every tooth lies the dental pulp, often referred to as the nerve of the tooth, although it is much more than just that. This soft, living tissue fills the pulp chamber in the crown and the root canal(s) extending down into the tooth’s root(s). The pulp is a complex mix of blood vessels, nerves, connective tissue, and specialized cells, most notably the odontoblasts we mentioned earlier, which line the periphery of the pulp chamber.
Vital Functions of the Pulp
The pulp has several vital functions. Firstly, it is responsible for sensory input. The nerves within the pulp transmit signals of pain, temperature, and pressure. While often associated with discomfort, this pain response is a crucial defense mechanism, alerting you when something is wrong, such as a deep cavity, infection, or injury. Secondly, the pulp provides nourishment to the tooth. The blood vessels supply the oxygen and nutrients necessary to keep the odontoblasts and other cells alive and functioning, allowing for the continued formation of dentin throughout life. This includes secondary dentin, which slowly forms after tooth eruption, and tertiary dentin in response to stimuli.
Thirdly, the pulp plays a formative role. During tooth development, it is the pulp that forms the dentin. The odontoblasts are the cells specifically responsible for this dentinogenesis. Finally, the pulp has a defensive and reparative capacity. If bacteria invade, the pulp can mount an inflammatory response, and as mentioned, odontoblasts can produce tertiary dentin to wall off the insult. However, if the pulp becomes severely inflamed (pulpitis) or infected, it can be extremely painful and may eventually die, necessitating root canal treatment or tooth extraction to prevent the spread of infection.
When decay reaches the pulp, or if the pulp is exposed due to trauma, it becomes highly vulnerable to bacterial infection. This situation can rapidly lead to an abscess, a painful collection of pus at the root of the tooth. Prompt dental attention is critical if you suspect pulp involvement to potentially save the tooth and prevent further health complications.
Anchoring the Foundation: Cementum
Moving down from the visible crown, we enter the realm of the tooth’s root, which is embedded within the jawbone. The outermost layer covering the root surface is cementum. This is a specialized, calcified connective tissue, somewhat softer than dentin but harder than bone. Its primary role is to provide a surface for the attachment of the periodontal ligament fibers, which anchor the tooth securely in its bony socket.
Cementum is yellowish and thinner near the cervical line, where enamel meets cementum at the neck of the tooth, and thicker towards the apex, the tip of the root. Unlike enamel, cementum is formed continuously throughout life. As we age, or in response to stress or wear, new layers of cementum can be deposited, particularly at the root apex. This ongoing deposition can help compensate for the slight wear that occurs on the chewing surfaces of teeth over time, helping to maintain the overall length of the tooth within the jaw.
There are two main types of cementum: acellular, or primary, cementum, which forms before the tooth reaches the occlusal plane, and cellular, or secondary, cementum, which forms after the tooth is in occlusion and contains cells called cementocytes. Cementum, like dentin, can undergo some repair if damaged, contributing to the tooth’s overall resilience.
The Tooth’s Suspension System: Periodontal Ligament
Nestled between the cementum of the tooth root and the alveolar bone of the jaw is a crucial structure called the periodontal ligament, or PDL. It is not a layer of the tooth itself, but rather a specialized connective tissue that acts like a sophisticated suspension system, holding the tooth in its socket. The PDL is composed of bundles of collagen fibers, known as Sharpey’s fibers, that insert into the cementum on one side and the alveolar bone on the other.
This ligamentous connection is not rigid; it allows for a tiny amount of tooth movement, which is essential for several reasons. It acts as a shock absorber, cushioning the tooth and jawbone from the forces of biting and chewing. This slight flexibility helps prevent damage to the tooth and surrounding bone. The PDL is also rich in nerves and blood vessels. The nerves provide proprioceptive feedback, meaning they help your brain sense how hard you are biting and the position of your teeth, allowing for fine control during mastication. The blood vessels supply nutrients to the cementum and alveolar bone, maintaining their health.
The Supportive Socket: Alveolar Bone
Surrounding and supporting the roots of the teeth is the alveolar bone, which is part of the maxilla, the upper jaw, and mandible, the lower jaw. The specific part of the alveolar bone that lines the tooth socket is called the lamina dura. The periodontal ligament fibers embed directly into this bone, creating a strong yet dynamic connection that is vital for tooth stability.
Alveolar bone is a living, constantly changing tissue. It responds to the forces placed upon it. For example, during orthodontic treatment, the gentle, sustained pressure from braces causes bone to resorb, or dissolve, on one side of the tooth root and new bone to form on the other, allowing teeth to be moved into new positions. If a tooth is lost and not replaced, the alveolar bone in that area may gradually resorb due to lack of stimulation. This highlights why dental implants are often recommended, as they can help maintain bone health by mimicking the presence of a natural tooth root.
The Protective Collar: Gingiva
While not technically a layer of the tooth itself, the gingiva, or gums, plays an indispensable role in protecting the tooth and its supporting structures. This soft tissue forms a collar around the neck of each tooth, sealing off the underlying bone and root from the oral environment. Healthy gums are firm, pink, and do not bleed easily. They form a critical barrier against bacteria, preventing them from reaching the periodontal ligament and alveolar bone. If this barrier is compromised, it can lead to gum disease, periodontitis, and eventual tooth loss. Maintaining healthy gums through regular brushing, flossing, and dental check-ups is just as important as caring for the teeth themselves.
So, the next time you brush your teeth, take a moment to appreciate the complex, multi-layered structures you are caring for. From the super-hard enamel shield to the living, responsive pulp, and the intricate network of supporting tissues like the periodontal ligament and alveolar bone, each component works in concert to allow us to eat, speak, and smile with confidence. Understanding these layers highlights the importance of comprehensive oral care, which aims to protect and maintain every part of this incredible natural system for a lifetime of health.