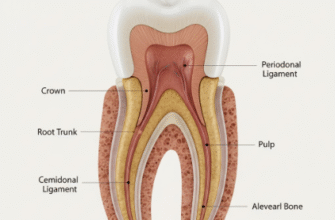
Often overshadowed by its more famous neighbors, enamel and dentin, cementum plays an indispensable, albeit quieter, role in the life and health of a tooth. This specialized, calcified connective tissue forms a thin layer covering the entire root surface, from the cementoenamel junction (CEJ) where it meets the enamel, down to the very tip, or apex, of the root. Think of it as a living interface, a crucial bridge connecting the tooth to the surrounding jawbone, ensuring stability and enabling the tooth to withstand the daily rigors of chewing and speaking.
Compositionally, cementum shares similarities with bone, containing about 45-50% inorganic mineral (primarily hydroxyapatite) and 50-55% organic matrix and water. The organic matrix is rich in collagen fibers, predominantly type I collagen, along with various non-collagenous proteins that orchestrate its formation and function. However, unlike bone, mature cementum is typically avascular, meaning it lacks its own blood supply, and it doesn’t usually undergo the same degree of continuous remodeling seen in bone tissue. This unique characteristic influences how it responds to stress and injury.
Understanding the Varieties of Cementum
Not all cementum is created equal. Dental professionals primarily distinguish between two main types, based on the presence or absence of cells within their matrix and the origin of their collagen fibers. These types often coexist on the same root surface, each tailored to specific functional demands.
Acellular Extrinsic Fiber Cementum (AEFC)
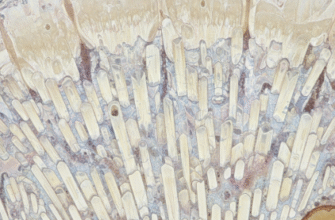
Acellular Extrinsic Fiber Cementum, often referred to as primary cementum, is the first type to be formed during tooth development. It covers approximately the cervical two-thirds of the root. As its name suggests, it is devoid of cells (cementocytes) within its calcified matrix. The “extrinsic fibers” are Sharpey’s fibers, which are the terminal ends of the principal collagen fibers of the periodontal ligament (PDL). These fibers originate in the PDL, run towards the root, and become embedded within the AEFC, anchoring the tooth firmly to the alveolar bone. This type of cementum is crucial for tooth attachment and is formed relatively slowly.
Cellular Intrinsic Fiber Cementum (CIFC)
Cellular Intrinsic Fiber Cementum, or secondary cementum, is typically found on the apical third of the root and in the furcation areas of multi-rooted teeth (the space between roots). Unlike AEFC, this type contains cells called cementocytes, which are entrapped cementoblasts, residing in spaces called lacunae, much like osteocytes in bone. The “intrinsic fibers” are produced by the cementoblasts themselves. Cellular cementum is formed more rapidly than acellular cementum and its primary roles are in adaptation and repair. It can increase in thickness throughout life, especially in response to wear or tooth movement, helping to maintain the length of the tooth and ensure occlusal harmony.
There’s also a variant known as mixed stratified cementum, which, as the name implies, exhibits alternating layers of acellular and cellular cementum. This is often seen in the apical regions and furcations, reflecting periods of varying functional demands and reparative activity.
The Repairman of the Root: Cementum’s Healing Touch
One of cementum’s most vital functions is its contribution to the repair of root surfaces following minor injuries. Teeth can experience various forms of damage, such as small fractures, resorption (a process where tooth structure is lost), or even minor trauma from dental procedures. When the root surface is damaged, specialized cells called cementoblasts play a crucial role in the healing process.
Cementoblasts are typically found lining the surface of the cementum, adjacent to the periodontal ligament. In response to injury or specific signaling molecules, these cells can be activated to synthesize and deposit new cementum matrix. This new matrix, initially unmineralized (called cementoid), gradually calcifies, attempting to restore the integrity of the root surface and re-establish a healthy connection with the periodontal ligament. This reparative cementum is usually of the cellular type, allowing for quicker deposition.
Cementum is a unique mineralized tissue essential for tooth anchorage and plays a significant role in root surface repair. Its ability to deposit new layers helps maintain periodontal ligament attachment and adapt to functional changes. This continuous, albeit slow, formation is vital for long-term tooth stability and health.
While cementum has this remarkable reparative capacity, it’s important to understand its limitations. The repair process is generally more effective for minor defects. Extensive damage or chronic inflammation, such as that seen in advanced periodontal disease, can overwhelm cementum’s ability to heal effectively. Furthermore, the regeneration of a perfectly structured and functionally integrated cementum-PDL complex remains a significant challenge in periodontal therapy.
An Anchor and Adaptor: Cementum’s Significance in Periodontal Stability
The health of the periodontium – the tissues supporting the tooth, including the gingiva, periodontal ligament, cementum, and alveolar bone – is fundamentally linked to the integrity and function of cementum.
Foundational Anchorage
Perhaps the most well-recognized function of cementum is providing firm anchorage for the periodontal ligament (PDL) fibers. As mentioned earlier, the collagen fibers of the PDL, known as Sharpey’s fibers, insert directly into the cementum on one side and the alveolar bone on the other. This intricate connection forms a strong yet flexible suspensory apparatus that holds the tooth within its socket. Without sound cementum, this vital attachment would be compromised, leading to tooth mobility and eventual loss. The AEFC, with its dense arrangement of embedded Sharpey’s fibers, is particularly critical for this function.
Adapting to Change
Teeth are not static structures; they are subject to various forces and can undergo movement throughout life. This includes physiological drift (mesial drift, where teeth tend to move slightly towards the front of the mouth over time), changes due to occlusal wear, and movement induced by orthodontic treatment. Cementum plays a key adaptive role in these scenarios. New layers of cellular cementum can be deposited, particularly at the root apex and in areas of tension, to compensate for tooth wear and to help maintain the width of the PDL during tooth movement. This adaptive deposition ensures that the tooth remains functional and properly positioned.
Protecting the Inner Sanctum
Cementum also serves as a protective barrier for the underlying dentin on the root surface. Dentin contains microscopic tubules that communicate with the tooth’s pulp. If the cementum layer is lost, due to gum recession or aggressive scaling, these dentinal tubules can become exposed to the oral environment, leading to tooth sensitivity to hot, cold, or sweet stimuli. A healthy, intact layer of cementum effectively seals these tubules, preventing such discomfort.
When Cementum Faces Adversity: Biological Responses and Considerations
Despite its resilience, cementum is not immune to challenges. Various factors can affect its integrity and function, leading to biological responses that impact tooth health.
The Phenomenon of Resorption
Cementum can undergo resorption, a process where it is broken down and lost. This can be triggered by several factors, including chronic inflammation (often associated with periodontal conditions), excessive occlusal forces (trauma from occlusion), pressure from impacted teeth or tumors, and sometimes as a side effect of orthodontic tooth movement if forces are too heavy or rapid. While some minor resorption can often be repaired by new cementum deposition once the stimulus is removed, extensive or persistent resorption can weaken tooth anchorage.
The Issue of Exposure
Gingival recession, where the gum tissue pulls away from the tooth, can lead to the exposure of root cementum to the oral environment. Exposed cementum is softer and thinner than enamel, making it more susceptible to wear from brushing and to decay (root caries). Furthermore, as mentioned, its loss can lead to dentin hypersensitivity. The junction where enamel meets cementum, the CEJ, is a particularly vulnerable area. In some individuals, there’s a small gap between enamel and cementum at the CEJ, leaving dentin exposed from the outset.
Cementum in the Context of Periodontal Changes
In situations of periodontal inflammation, the surface characteristics of cementum can be altered. Bacterial plaque accumulation on the root surface can lead to the release of endotoxins and other byproducts that may penetrate the cementum. This can make the cementum surface less hospitable for the reattachment of periodontal ligament cells, complicating healing processes if the inflammation is not controlled. Understanding these interactions is key to appreciating the complex nature of periodontal health and disease, where cementum plays a passive but important role as a surface affected by the surrounding biological environment.
Occasionally, an overgrowth or excessive formation of cementum, known as hypercementosis, can occur. This condition can thicken the root, sometimes making tooth extraction more difficult if needed. It’s often idiopathic (of unknown cause) but can sometimes be associated with chronic low-grade inflammation, non-functional teeth, or certain systemic conditions.
A Lifelong Process: The Dynamic Nature of Cementum
A fascinating aspect of cementum is its capacity for continuous, albeit slow, deposition throughout an individual’s life. Unlike enamel, which ceases formation once the tooth erupts, cementum production can continue, particularly the cellular type. This ongoing process allows the tooth to adapt to changing functional demands and to attempt repair of minor surface damage. With age, the overall thickness of cementum, especially in the apical and furcation areas, tends to increase. This is a natural adaptive mechanism. The outermost layer of cementum is often a thin, unmineralized layer called cementoid, which represents the most recently formed matrix before it undergoes calcification. This dynamic nature underscores cementum’s role as a living tissue, constantly interacting with its environment within the periodontium.
This continual apposition helps to maintain the tooth’s functional length, compensating for the slight occlusal wear that occurs over many years of use. It also ensures that the periodontal ligament fibers remain securely embedded, even as the older layers of cementum might undergo subtle surface changes. This ability to add new layers is a testament to the sophisticated design of the dental apparatus, where each component contributes to long-term function and durability.