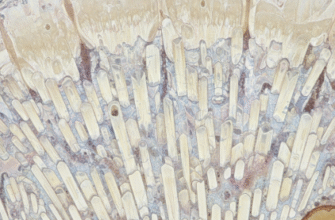
Ever run your tongue over your teeth and felt that slightly fuzzy, sometimes even gritty, film? That, my friend, is dental plaque. And while it might seem like just a bit of leftover lunch, it’s a far more fascinating and complex world than you might imagine. It’s not just inert debris; it’s a living, breathing (in some cases, quite literally) community of microorganisms. We’re talking about a biofilm, a highly organized and cooperative society of countless bacteria, all shacked up together on your pearly whites.
Think of it less like a random scattering of dust bunnies and more like a miniature, bustling metropolis, complete with diverse neighborhoods, communication systems, and even its own architectural structures. This “fun fact” – that plaque is a biofilm – changes how we understand what’s happening in our mouths every single second.
So, What Exactly is a Biofilm?
The term “biofilm” might sound like something out of a science fiction movie, but it’s a very real and very common phenomenon in nature. At its core, a biofilm is a collective of one or more types of microorganisms that can grow on many different surfaces. Microorganisms in biofilms include bacteria, fungi, and protists. What makes them special is their organization. They don’t just float around independently; they adhere to surfaces and, crucially, to each other. And they build themselves a protective home.
This home is typically a slimy, glue-like substance called an Extracellular Polymeric Substance (EPS) matrix. Imagine it as the cement and scaffolding of their microbial city. This matrix, which the bacteria themselves produce, helps them stick together, protects them from environmental threats (like being washed away or changes in temperature or pH), and can even help them trap nutrients. You’ve seen biofilms elsewhere: the slippery coating on rocks in a stream, the gunk that can build up inside pipes, or even the film on an old vase of flowers. Dental plaque is simply one of the most well-known and personally relevant examples of this natural microbial lifestyle.
Living in a biofilm offers significant advantages to bacteria. It provides:
- Protection: The EPS matrix shields them from harm.
- Adhesion: It helps them stay put in a desirable location, like a nutrient-rich tooth surface.
- Nutrient capture: The matrix can trap nutrients from the surrounding environment.
- Cooperation: Bacteria within a biofilm can communicate (a process called quorum sensing) and even share resources or tasks, making the community more resilient and efficient than individual bacteria would be on their own.
A Microscopic Menagerie: The Bacteria in Plaque
Dental plaque isn’t a monotonous landscape populated by a single type of bacterium. Oh no, it’s a veritable melting pot of hundreds, yes, hundreds of different bacterial species, each with its own role and characteristics. It’s like a diverse ecosystem, with different organisms thriving at different stages of the biofilm’s development and in different micro-environments within the plaque structure itself.
The cast of characters changes as the plaque biofilm matures. Initially, you have the early colonizers. These are often aerobic bacteria (oxygen-loving) like certain species of Streptococcus (e.g., Streptococcus sanguinis, Streptococcus oralis, and Streptococcus mitis) and Actinomyces. These pioneers are good at sticking to the initial conditioning film that forms on teeth (more on that soon). They are like the first settlers in a new land, laying the groundwork for others to follow.
As these early colonizers multiply and start to build the EPS matrix, they change the local environment. Oxygen levels might decrease deeper within the growing plaque layer. This creates opportunities for secondary or later colonizers to move in. Many of these are anaerobic (thriving in low-oxygen or oxygen-free conditions) or facultative anaerobic (can live with or without oxygen). Species like Fusobacterium nucleatum are famous for being “bridging” organisms, meaning they can coaggregate (stick to) both early and other late colonizers, helping to build more complex structures. Other later arrivals can include bacteria like Porphyromonas gingivalis, Tannerella forsythia, and various spirochetes. As the biofilm thickens and matures, the population becomes more diverse and, often, more dominated by anaerobic species, especially in the deeper layers closest to the tooth surface.
Dental plaque is indeed a complex biofilm, a well-established scientific fact. It’s a bustling city of microbes, not just a random collection of leftover food. Scientists have studied its intricate structure and diverse microbial composition extensively. Understanding this biological phenomenon helps us appreciate the dynamic nature of the oral environment.
The Step-by-Step Construction of a Microbial City
The formation of dental plaque is not a haphazard event; it’s a surprisingly orderly, multi-stage process. It’s like watching a tiny city being built in fast-forward, right there on your teeth.
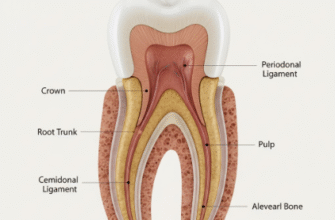
Stage 1: Pellicle Power!
Almost immediately after your teeth are cleaned, a very thin, invisible layer called the acquired pellicle forms on the tooth enamel. This isn’t bacteria; it’s made up of proteins and glycoproteins from your saliva. Think of it as the pristine, undeveloped land upon which our microbial city will be built. It’s the foundation, the primer coat that makes the tooth surface more receptive to bacterial attachment.
Stage 2: The First Settlers Arrive (Initial Attachment)
Next, the pioneer bacteria, those early colonizers we mentioned, begin to attach to this pellicle. This initial attachment is often loose and reversible – the bacteria can still be easily dislodged. However, if they’re not disturbed, they’ll start to anchor themselves more firmly using specific adhesion molecules on their surfaces that bind to receptors in the pellicle.
Stage 3: Building Boom (Multiplication and Coaggregation)
Once firmly attached, these early colonizers begin to multiply. They grow and divide, forming microcolonies. Simultaneously, they start producing that all-important EPS matrix – the slime that will hold everything together. This is also when coaggregation kicks into high gear. The early colonizers display receptors on their surfaces that other bacteria (the later colonizers) can recognize and bind to. It’s like bacteria holding hands with other bacteria, creating complex, multi-species aggregates. This is how the biofilm starts to grow in thickness and complexity.
Stage 4: Maturation of the Metropolis and Spreading the Word
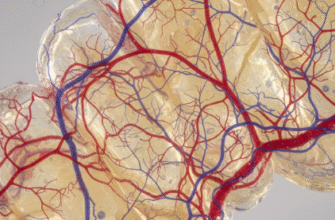
As more bacteria join and the EPS matrix develops, the biofilm matures. It becomes a highly organized, three-dimensional structure. You might find channels within the plaque that allow nutrients to flow in and waste products to flow out – a primitive circulatory system! The environment within the biofilm also changes. Deeper layers become anaerobic, favoring different types of bacteria than those on the surface. Communication between bacteria (quorum sensing) becomes sophisticated, allowing them to coordinate their activities. Finally, at certain points, bits of the biofilm may detach, and individual bacteria or clumps of bacteria can be released to colonize new surfaces in the mouth, starting the process all over again. It’s a dynamic, ever-changing structure.
Why This “Sticky” Situation Matters
Understanding that dental plaque is a well-structured biofilm, rather than just a smear of bacteria, is crucial. The biofilm nature explains why it’s so tenacious and persistent. That EPS matrix isn’t just a passive goo; it’s a shield. It protects the bacteria nestled within from things like your saliva’s natural antibacterial components, from sudden pH changes (like when you eat something acidic), and even, to some extent, from the active ingredients in some oral hygiene products if the biofilm is very thick and mature. It’s this organized, protected structure that makes plaque a challenge.
The community aspect is also key. Different bacteria within the biofilm can have synergistic relationships. One type might break down complex sugars into simpler forms that another type can then use for energy. This metabolic cooperation makes the community more efficient and resilient. The close proximity also allows for the transfer of genetic material between bacteria, which can spread traits like antibiotic resistance (though this is more a concern in other types of biofilms relevant to infections, the principle of genetic exchange in dense communities is important).
Keeping the Microbial Tenants in Check
So, if plaque is such a sophisticated and well-defended microbial city, what can be done? The primary strategy for managing dental plaque revolves around mechanical disruption. Because it’s a physical structure, it needs to be physically broken apart and removed.
This is where good old-fashioned brushing and flossing come into play. Brushing helps to scrub away the biofilm from the accessible surfaces of your teeth. Flossing, or using interdental cleaners, is vital for disrupting the plaque that forms between teeth and under the gumline, areas your toothbrush bristles can’t easily reach. The goal is to regularly disturb and remove these developing microbial communities before they can mature into highly complex and robust biofilms.
Think of it like regularly weeding a garden. If you do it frequently, you’re just removing small, easily managed seedlings. If you let the weeds grow for a long time, they develop deep roots and become much harder to eradicate. Similarly, disrupting plaque when it’s in its early stages of formation is much more effective. It’s not about achieving a sterile mouth – that’s neither possible nor desirable, as many oral bacteria are harmless or even beneficial. It’s about controlling the accumulation and maturation of these biofilm communities to maintain a balanced oral environment.
The fact that dental plaque is a biofilm underscores the marvels of the microbial world. These tiny organisms are capable of incredible feats of engineering and cooperation, building complex societies right under our noses (or, more accurately, in our mouths!). It’s a daily reminder of the intricate dance of biology happening all around us, and within us.